What is Systemic Oppression?
Understanding The Framework Of Oppression
A common misconception is that institutional oppression (which is also sometimes called systemic oppression) is merely laws against a certain group of people. In reality it is often much more complex than that; institutional oppression takes form in various systems within society. This could be the legal system, the medical system, the educational system, and more. In order to understand the framework of oppression, many activists use “The Four I’s Of Oppression” by The Chinook Fund. The definition given of institutional oppression is “the idea that one group is better than another group and has the right to control the other gets embedded in the institutions of the society--the laws, the legal system and police practice, the education system and schools, hiring policies, public policies, housing development, media images, political power, etc”. The full document is attached below.Contact @asexualresearch on Twitter or [email protected] for articles that should be added, questions, or concerns!
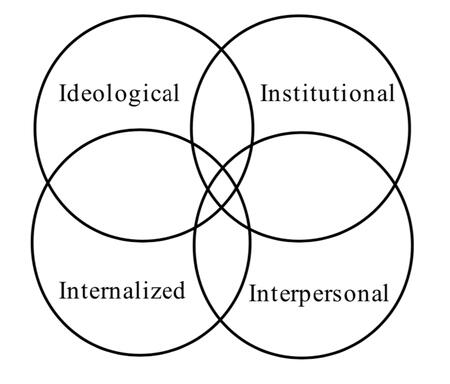
THE FOUR "I's" OF OPPRESSIONIdeological Oppression
First, any oppressive system has at its core the idea that one group is somehow better than another, and in some measure has the right to control the other group. This idea gets elaborated in many ways-- more intelligent, harder working, stronger, more capable, more noble, more deserving, more advanced, chosen, normal, superior, and so on. The dominant group holds this idea about itself. And, of course, the opposite qualities are attributed to the other group--stupid, lazy, weak, incompetent, worthless, less deserving, backward, abnormal, inferior, and so on.Institutional Oppression
The idea that one group is better than another group and has the right to control the other gets embedded in the institutions of the society--the laws, the legal system and police practice, the education system and schools, hiring policies, public policies, housing development, media images, political power, etc. When a woman makes two thirds of what a man makes in the same job, it is institutionalized sexism. When one out of every four African-American young men is currently in jail, on parole, or on probation, it is institutionalized racism. When psychiatric institutions and associations “diagnose” transgender people as having a mental disorder, it is institutionalized gender oppression and transphobia. Institutional oppression does not have to be intentional. For example, if a policy unintentionally reinforces and creates new inequalities between privileged and non-privileged groups, it is considered institutional oppression.Interpersonal Oppression
The idea that one group is better than another and has the right to control the other, which gets structured into institutions, gives permission and reinforcement for individual members of the dominant group to personally disrespect or mistreat individuals in the oppressed group. Interpersonal racism is what white people do to people of color up close--the racist jokes, the stereotypes, the beatings and harassment, the threats, etc. Similarly, interpersonal sexism is what men do to women-- the sexual abuse and harassment, the violence directed at women, the belittling or ignoring of women's thinking, the sexist jokes, etc.
Most people in the dominant group are not consciously oppressive. They have internalized the negative messages about other groups, and consider their attitudes towards the other group quite normal.
No "reverse racism". These kinds of oppressive attitudes and behaviors are backed up by the institutional arrangements. This helps to clarify the confusion around what some claim to be "reverse racism". People of color can have prejudices against and anger towards white people, or individual white people. They can act out those feelings in destructive and hurtful ways towards whites. But in almost every case, this acting out will be severely punished. The force of the police and the courts, or at least a gang of whites getting even, will come crashing down on those people of color. The individual prejudice of black people, for example, is not backed up by the legal system and prevailing white institutions. The oppressed group, therefore, does not have the power to enforce its prejudices, unlike the dominant group.
For example, the racist beating of Rodney King was carried out by the institutional force of the police, and upheld by the court system. This would not have happened if King had been white and the officers black.
A simple definition of racism, as a system, is: RACISM = PREJUDICE + POWER.
Therefore, with this definition of the systemic nature of racism, people of color cannot be racist. The same formula holds true for all forms of oppression. The dominant group has its mistreatment of the target group embedded in and backed up by society's institutions and other forms of power.Internalized Oppression
The fourth way oppression works is within the groups of people who suffer the most from the mistreatment. Oppressed people internalize the ideology of inferiority, they see it reflected in the institutions, they experience disrespect interpersonally from members of the dominant group, and they eventually come to internalize the negative messages about themselves. If we have been told we are stupid, worthless, abnormal, and have been treated as if we were all our lives, then it is not surprising that we would come to believe it. This makes us feel bad.
Oppression always begins from outside the oppressed group, but by the time it gets internalized, the external oppression need hardly be felt for the damage to be done. If people from the oppressed group feel bad about themselves, and because of the nature of the system, do not have the power to direct those feelings back toward the dominant group without receiving more blows, then there are only two places to dump those feelings--on oneself and on the people in the same group. Thus, people in any target group have to struggle hard to keep from feeling heavy feelings of powerlessness or despair. They often tend to put themselves and others down, in ways that mirror the oppressive messages they have gotten all their lives. Acting out internalized oppression runs the gamut from passive powerlessness to violent aggression. It is important to understand that some of the internalized patterns of behavior originally developed to keep people alive--they had real survival value.
On the way to eliminating institutional oppression, each oppressed group has to undo the internalized beliefs, attitudes, and behaviors that stem from the oppression so that it can build unity among people in its group, support its leaders, feel proud of its history, contributions, and potential, develop the strength to challenge patterns that hold the group back, and organize itself into an effective force for social change.Internalized Privilege
Likewise, people who benefit the most from these systems internalize privilege. Privileged people involuntarily accept stereotypes and false assumptions about oppressed groups made by dominant culture. Internalized privilege includes acceptance of a belief in the inherent inferiority of the oppressed group as well as the inherent superiority or normalcy of one’s own privileged group. Internalized privilege creates an unearned sense of entitlement in members of the privileged group, and can be expressed as a denial of the existence of oppression and as paternalism.It should be clear that none of these four aspects of oppression can exist separately. As the diagram [above] suggests, each is completely mixed up with the others. It is crucial at see any oppression as a system. It should also be clear that trying to challenge oppression in any of the four aspects will affect the other three.”
What Is Compulsory Sexuality?
The Systemic Privileging of Allosexuality
Compulsory sexuality (also call amanormativity or sexusociety) is "the assumption that all people are sexual and to describe the social norms and practices that both marginalize various forms of nonsexuality and compel people to experience themselves as desiring subjects, take up sexual identities, and engage in sexual activity" (Gupta). Several scholars have begun to take an in-depth look into this field of study.All sources will be uploaded under the Works Cited page.Contact @asexualresearch on Twitter or [email protected] for articles that should be added, questions, or concerns!
Exploring the Experiences of Heterosexual and Asexual Transgender People (The University of Tampa And Vanderbilt University)
“Asexual organizing also presents a challenge to asexual discrimination. Researchers across fields have provided evidence for “asexphobia” or “anti- asexual bias/prejudice” such that asexuals are understood as “deficient,” “less human, and disliked.”28 Asexphobia exists at the level of attitudes that have negative effects on asexual people such as when they are interrogated and asked intrusive questions about their bodies and sexual lives, or when they are presented with “denial narratives” to undermine the validity of their asexual- ity.29 In figure 0.2, from the zine Taking the Cake, Maisha indicates the many ways in which asexuality can be undermined. For example, people might sug- gest that an ace person is repressed, closeted, incapable of obtaining sex from others, or in an immature phase. These dismissive comments are informed by ableist ideas, such as that disability prevents the capacity for sex and that ability rests on an enjoyment of and desire for sex as well as by compulsory sexuality, which suggests that sex is necessary, liberatory, and integral to hap- piness and well-being. Discrimination can also take on the form of social and sexual exclusion, including in queer contexts: through “conversion” practices in medical and clinical environments to encourage asexuals to have sex, with unwanted and coerced sex in partner contexts, through the misdiagnosis of sexual desire disorders in people who are asexual, and with invisibility, toxic attention, or the fetishization of asexual identity.31 Recognizing discrimina- tion is important because it refuses to see individual acts against asexuals as incidental, providing a systemic view on patterns of “dislike” against asexuals.“
Crisis and safety: The asexual in sexusociety (American Psychological Association)
"The ‘sexual world’ is for asexuals very much akin to what patriarchy is for feminists
and heteronormativity for LGBTQ populations, in the sense that it constitutes the
oppressive force against which some sort of organizing and rebellion must take 4
place.To be quite a bit more specific, what are sexusociety’s favoured repetitions? Despite the diversity of feminist articulations on this topic (in other words the topic of what patriarchy ‘wants’ us to do), most feminists would likely give a similar answer: coital sex, sex with a purpose (be it reproduction or male orgasm), heterosexual and heteronormative sex, sex within marriage or coupledom, the importance of two, and a sexuality that amounts to little more than the sum of these. Gayle Rubin deems this a ‘hierarchical system of sexual value’, outlining textually and pictorially which acts are privileged and which collectively feared and despised (2006 [1984]: 529). Most relevant for this discussion of asexuality, however, is the favoured repetition of sex, understood mostly in a coital and heteronormative sense, and the compulsion to repeat sexually, as opposed to say intellectually (though I am not saying that the two do not overlap and interlace).These snippets of our cultural necessity to have sex, most prefer- ably heterosexually and coitally, are relevant to this discussion of asexuality because it is against such normative scripts of sexual repetition that pathologies of non-sex are constructed.In a certain sense, the absence of sexual ‘urges’ becomes more problematic
than an overabundance of them, as is strangely crystallized by a triad of sexologists in 1998 who ‘plead for the introduction of a category on excessive (or hyperactive) sexual desire’, whereas the addition of new and varied sexual lack pathologies does not need to be pleaded for (Vroege et al., 2001: 239). And as Gavey suggests, the problem may not lie in disordered women, so much as in a lack of interest in the sex that is being repeated as ‘normal’, ‘the kind of sex on offer’ (2005: 112). Leonore Tiefer reminds us that we should be wary of regarding the DSM as a neutral source indexing reality, but remember instead that it is itself a cultural production invested in a gendered and heterosexist system (1995: 97–102).This impetus to pathologize those who are not sexual enough, or who do not repeat sexuality faithfully to ‘the norm’, is indicative of which repetitions are favoured by sexusociety. But it also, and more relevantly, embodies sexusociety’s interest in maintaining a society that repeats along sexual lines.David Jay is subsequently coerced to reveal details of his asexuality, he is positioned as an object of sexual lack and is altogether bewildering for the hosts (Jay, 2007b). He must disclose details of his non-sexual past (‘do you masturbate?’) so that the hosts and the audience may assess to what extent his ‘non’-sexuality is ‘true’ (and of course, faithful repetition is impossible and any detail from the past may be fished out as counterevidence to his claims).It also demonstrates sexusociety’s employ- ment of the confession as a means to correct incorrect repetition. So while David Jay confesses absence, the hosts strive to reconfigure absence into a sexual presence that resembles the ideal, in this case, the sexual ideal. Improper sexual repetitions (or in the case of asexuality, the paucity of sexual repetitions) are remedied with the guidance of other sexual subjects who are more faithful to the norms of sexual acting (presumably the hosts of The View). The confession is thus one of those very special moments within sexusociety when wrongs may be righted, when faulty repetitions may be discouraged or made to appear fraudulent, and when difference or absence may be permutated into a correct presence. Sex, and now also its absence, ‘has to be put into words’ (Foucault, 1990 [1978]: 32).Asexuality would do well to recognize that there is no vacation away from sexusocial discourse; even the micro safe space of the asexual body is in fact embedded within sexusociety. "
Lessons from bisexual erasure for asexual erasure (University of Amsterdam)
"Bisexual erasure is undoubtedly powerful; however, certain points made within this essay could lead one to conclude that asexual erasure must be even more oppressive. Asexuality does not stop at changing the rules of the game of sexuality as bisexuality does, but broadly refuses to even play the game. It is not that sex is undermined because the asexual is simply sex blind (a blindness which, incidentally, is greater than that sex blindness found in bisexuals); rather, sex is undermined since the private erotic realm that produces and sustains it does not exist for the asexual. And it is not so much monogamy that is threatened by asexuality (though the sexual dynamics within it are), but instead intimate relationships in general – a threat presented most acutely by the aromantic asexual. Such is the more important destabilising power of asexuality for the norms allosexuality would have preserved, and consequently greater is the erasure asexuality ought to receive."
Asexual (GLOBAL ENCYCLOPEDIA OF LESBIAN, GAY, BISEXUAL, TRANSGENDER, AND QUEER HISTORY)
“Asexual organizing also presents a challenge to asexual discrimination. Researchers across fields have provided evidence for “asexphobia” or “anti- asexual bias/prejudice” such that asexuals are understood as “deficient,” “less human, and disliked.”28 Asexphobia exists at the level of attitudes that have negative effects on asexual people such as when they are interrogated and asked intrusive questions about their bodies and sexual lives, or when they are presented with “denial narratives” to undermine the validity of their asexual- ity.29 In figure 0.2, from the zine Taking the Cake, Maisha indicates the many ways in which asexuality can be undermined. For example, people might sug- gest that an ace person is repressed, closeted, incapable of obtaining sex from others, or in an immature phase. These dismissive comments are informed by ableist ideas, such as that disability prevents the capacity for sex and that ability rests on an enjoyment of and desire for sex as well as by compulsory sexuality, which suggests that sex is necessary, liberatory, and integral to hap- piness and well-being. Discrimination can also take on the form of social and sexual exclusion, including in queer contexts: through “conversion” practices in medical and clinical environments to encourage asexuals to have sex, with unwanted and coerced sex in partner contexts, through the misdiagnosis of sexual desire disorders in people who are asexual, and with invisibility, toxic attention, or the fetishization of asexual identity.31 Recognizing discrimina- tion is important because it refuses to see individual acts against asexuals as incidental, providing a systemic view on patterns of “dislike” against asexuals.“
Asexual Erotics
"Researchers across fields have provided evidence for “asexphobia” (Kim 2014) or “anti-asexual bias/prejudice” such that asexuals are understood as “deficient,” “less human, and disliked” (MacInnis and Hodson 2012, 740). Asexphobia exists at the level of attitudes that have negative effects on asexual people when they are interrogated and asked intrusive questions about their bodies and sexual lives, or when they are presented with “denial narratives” to undermine the validity of their asexuality (MacNeela and Murphy 2015). Discrimination can also take the form of social and sexual exclusion, including in queer contexts; through “conver- sion” practices in medical and clinical environments to encourage asexuals to have sex; with unwanted and coerced sex in partner contexts; through the misdiagnosis of sexual desire disorders in people who are asexual; and with invisibility and toxic attention or the fetishization of asexual identity (Ginoza et al. 2014; Przybylo 2014; Chasin 2015; Cerankowski 2014). Recognizing discrimi- nation is important because it refuses to see individual acts against asexuals as incidental, providing a systemic view on patterns of “dislike” against asexuals.Third, queer and feminist research definitions of asexuality also place asexuality in direct dialogue with larger power structures and patterns of injustice. Devel- oping the important term compulsory sexuality by drawing on the work of the legal scholar Elizabeth F. Emens (2014), Kristina Gupta (2015) elaborates on the ways in which compulsory sexuality is a system that encourages some people to have sex, even while banning marginalized groups from sexual expression through the process of “desexualization.” “Sexusociety,” or a society organized around sex (Przybylo 2011), partakes in desexualization, as Kim’s work explores, to render marginalized groups such as people with disabilities, lesbians and transgender people, children and older adults, people of size, and some racialized groups as “asexual” by default—misusing the term asexuality in the process. For example, transgender people have historically needed to feign asexuality and demonstrate disgust for homosexual sex in order to have their surgeries approved and their trans identities confirmed as “valid” by medicine (Valentine 2007). More broadly, desexualization ranges from discourses around people with disabilities not being capable of sex or not being desirable to eugenics-based initiatives for managing a population through controlling reproduction via methods of coerced sterilization.
Desexualization and compulsory sexuality are also linked to hypersexualization, or the branding of some groups and most especially gay men and racialized groups as excessively sexual and lascivious and thus in need of population management. Treatment of people with AIDS in the 1980s, for example, and the pivoting of the “AIDS epidemic” as “God’s punishment for being gay” demonstrate how the deployment of hypersexualization, in combination with homophobia, can have lethal effects on marginalized groups. Ianna Hawkins Owen (2014) discusses how compulsory sexuality has uneven racial histories, such that whiteness has tended to emulate an “asexuality-as-ideal” as demonstrative of a form of innocence, moral control, and restraint, whereas black people have often been positioned as hypersexual so as to justify chattel slavery, lynching, and other instruments of racism. Hypersexualization and desexualization have thus been used historically and are in the present used as forms of social control and oppression, toward the maintenance of a white, able-bodied, hetero- patriarchal nation-state. Feminist and queer research on asexuality thus invites examinations of the intersectional histories and present-day realities of compulsory sexuality."
The Violence of Heteronormative Language Towards the Queer Community
“ Asexuality is a spectrum that is characterized by a lack of sexual attraction to other people; asexuals might still experience romantic attraction to others, or they might not, in which case they would also be aromantic. In attempting to “explain” their sexuality in ways that fit heteronormative standards, asexuals can unintentionally contribute to their own erasure.
Common ways of trying to make asexuality accessible to a heterosexual audience include saying that “asexuals are just like everyone else, but without the sex” or explaining asexuality in terms of food— for example, some people like and crave cake, while others do not. This metaphor is problematic as it implies that asexuality is only a minor aspect of one’s personality, as easily removed or overlooked as one’s food preferences. Similarly problematic are discussions of sexual attraction in society at large (particularly in the context of masculinity) that assert that attraction is a necessary part of the human experience.
These kinds of definitions put asexuals in an uncomfortable spot. Under heteronormativity, they would not be considered “normal” and might not easily fit into other heteronormative categories (for example, an asexual could be transgender and homoromantic, and thus would not easily fit into the heteronormative mold). For this reason, asexuals feel the need to liken themselves to heterosexuals and prove that they are “normal” and can fit in. The implications of such statements are that everyone else in the queer community is somehow abnormal or not like “everyone else.”
Such analogies present asexuality as a watered- down version of another sexuality—heterosexuality lite, so to speak—erasing asexual experiences. This
is a form of heteronormative language violence, as it can cause asexuals to be pushed away from the broader queer community because their deviance from the heteronormative standard may not be as immediately obvious as, for example, a homosexual transgender person’s might. In addition, as a result of the language above, “gate-keeping” within the asexual community can arise, where some are excluded because they do not seem “queer enough”—for example, a heteroromantic demisexual (a sexuality on the asexual spectrum where one can feel sexual attraction to another ONLY after a strong emotional bond has been formed) could “pass” as straight, and thus might be seen as not needing the support of the community (Asexual 1). After all, if they were “just like everyone else” then why would they need a special community for support?
Though isolated from the LGBTQIA community (a community perhaps best suited to understand the experience of living in a world that sets a certain pattern of behavior and feelings that they do not share as “normal”) asexuals will not necessarily find the support they need in the broader heteronormative context of society.
Heteronormative language is violent, as it diminishes the identity of bisexuals and asexuals while limiting their ability to find support within the communities that are best suited to their experiences. Heteronormative language also denies asexuals the ability to express their experiences without being questioned, and invalidates the asexual identity—a form of violence. Similar to the argument that bisexuals are “confused” or “halfway in the closet,” the oversimplification of the asexual identity through cute analogies implies that asexuality is a quirk or a phase, rather than a valid identity and a major part of a person’s personality. Language that trivializes asexuality limits the ability of asexuals to express themselves, their experiences and their sexuality without fear of repercussions, whether that is not being taken seriously or being treated as an outsider. It normalizes the idea that heterosexuality is “normal” and preferable to any other orientation, to the point where those who identify differently must prove how like heterosexuals they are to be afforded respect. Thus, the erasure of asexuals and bisexuals is a form of heteronormative language violence. (Asexual 1)”
A mystery wrapped in an enigma – asexuality: a virtual discussion
“My general impression from the U.S. context is that the negativity directed at asexual individuals is similar in some ways to the negativity directed at other sexual (and gender) minorities: asexual individuals, like other sexual minorities, may be perceived as mentally or physically ill, asexual individuals may feel alienated in social settings organized to facilitate heterosexual coupling, and asexual individuals may be denied legal and/or social recognition of their most important relationships. On the other hand, to a perhaps greater extent than other sexual minorities, asexual individuals are often denied ‘epistemic authority’ in regards to their own (a)sexuality. In other words, asexual individuals may be met with the reaction that they can’t really know that they are asexual – maybe they haven’t met the right person yet, maybe they are ‘late bloomers,’ maybe they are unconsciously repressing their sexual desires, maybe there is a physical cause of their asexuality that simply hasn’t been found yet.”
Towards a Historical Materialist Concept of Asexuality and Compulsory Sexuality
Theoretical Issues in the Study of Asexuality
“Simultaneously, the unquestioned presumption of the sexual norm—of sexuality as the norm—dictates that asexual people will very frequently pass as sexual people in everyday lives whether they want to or not. Asexual people therefore live an analogous biculturalism to the one Brown described of lesbians and gay men, and so incorporating the perspectives of asexual people into the domain of sexuality research could have corresponding benefits, as would engaging in alternative forms of inquiry, including qualitative investigations (as is already beginning). This is particularly the case with research related to sexual behavior, identity, and intimate relationships, since these (for anyone) are complex phenomena where subjective experiences are meaningful. Exploring asexual people’s subjective realities will help researchers come to a better understanding not only of asexuality, but of sexuality more generally. Doing so through the use of qualitative methodologies will permit researchers to begin exploring the pervasiveness of the sexualnormativity12 that would otherwise remain invisible in sexuality-related research.”
Why sexual people don’t get asexuality and why it matters (A personal essay written by Mark Carrigan, an allosexual researcher of asexuality)
“ I had three initial aims with my asexuality research: mapping out community in a ideographically adequate way, understanding the role the internet played in the formation of the community and exploring what the reception of asexuality reveals about sexual culture. There’s still more I want to write in relation to the first two points but I’ve basically drawn my conclusions at this point. Which means that my interest in asexuality has basically transmuted into an interest in how sexual people react to asexuality. This sounds much more obscure than it actually is.
In essence I’m arguing that the reactions of sexual people to asexuality reveal the architectonic principle of contemporary sexual culture, namely the sexual assumption: the usually unexamined presupposition that sexual attraction is both universal (everyone ‘has it’) and uniform (it’s fundamentally the same thing in all instances) such that its absence must be explicable in terms of a distinguishable pathology. This is instantiated at the level of both the cultural system and socio-cultural interaction: it’s entailed propositionally, even if not asserted outright, within prevailing lay and academic discourses pertaining to sexuality but it’s also reproduced by individuals in interaction (talking about sex, either in the abstract or in terms of their own experience) and intraaction (making sense of their own experience through internal conversation).
Until the asexual community came along, the ideational relationship (the logical structure internal to academic and lay discourses about sex) and patterns of socio-cultural interaction (the causal structure stemming from thought and talk about sex) reinforced one another. Or to drop the critical realist terminology: the sexual assumption got reproduced at the level of ideas because nothing conflicted with it at the level of experience. But when something comes along which empirically repudiates it (namely the asexual community) the underlying principle suddenly becomes contested. This doesn’t mean discourse ‘makes’ sexual people not get ‘asexuality’ but it does mean that, given the centrality of the sexual assumption to our prevailing ways of understand sexuality, being confronted with asexuality immediate invites explanation. One such explanation is to drop the ideational commitment but, given that its usually tacit, few people (including myself) can do this immediately – though many, it seems, do so once they’ve reflected upon it. Instead the usual response is to evade the logical conflict by explaining away asexuality: its a hormone deficiency, the person was sexually abused, they’re lying, they’re gay but repressed, they’ve just not met the right person yet (etc).
The empirical evidence of quite how pervasive, indeed near universal, this kind of reaction is seems increasingly conclusive. What I am suggesting is that the sexual assumption is what explains this being a ‘kind’ of reaction i.e. all the explanations, in spite of their superficial differences in content, involve a reassertion of the uniformity and/or universality of sexual attraction. I’m not saying people are deliberately or consciously defending the sexual assumption (though I’m not categorically saying no one will ever be doing this) but rather that it is this, as the foundational assumption ‘holding together’ the conceptual architecture of the sexual culture which has emerged from the mid/late 20th century onwards, which asexuality renders problematic. The precise content of any given individual’s attempts to explain away asexuality varies depending on the specifics of their personal and intellectual history within this sexual culture (i.e. it’s not a homogenous thing) but the shared form of the response is explained by the architectonic principle of that culture and the logical relation of contradiction in which it stands to the empirical observation of asexual individuals who are ‘normal’ (i.e. non pathological). Logical relations don’t force people to act (some people don’t try and explain it away) but everyone who has not experienced what David Jay calls the ‘head-clicky thing’ has the same initial reaction. The above is my first attempt to offer a convoluted social theorists explanation of what I mean when, in interviews, I talk about sexual people not ‘getting’ asexuality. If you follow my chain of reasoning then, I ask of you, test it out: go and read the comments on the Guardian article I linked to and think about the reactions of people on there and what they have in common. Or do the same with pretty much any news article which has comments that I’ve encountered. There is something really fucking interesting happening there.”
A research programme for queer studies
“But it is (or at least, it should be) clear that an asexual person’s relationship, both logical and existential, with the categories of sexuality and gender is deeply different from that of, say, a bisexual person: a bisexual person could find it difficult to affirm their own definition of their sexuality in a num- ber of social situations and relationships, and could as a consequence be a victim of marginalization, discrimination or violence; but for an asexual person the category of sexuality is simply not relevant: to compel an asexual person to position themselves along this category is, quite simply, nothing but a new form of oppression: and this form of oppression is even more insidious than the one which dominant heteronormativity exerts towards sexual minorities. First of all, because it is paradoxically justified as a form of liberation; but most of all because the “orthodox” and the “deviants”, in the field of sexuality and gender as in all others, share at least an orientation towards the world and a definition of priorities; both the inquisitor and the heretic place faith and dogma at the core of their self-definition. But that a person for whom the category of sexuality has no relationship to their lived experience and self-perception should be offered, as a form of liberation, the possibility to “integrate” in, and “be represented” by, a movement defined by the centrality and productivity of the category of sexuality and of all experiences (both positive and negative) which arise from it, is more or less equivalent to offering a person with no interest whatsoever in soccer the possibility to “integrate in society” by “coming out” as a supporter of some team, and of attending their games every Sunday.“
Marginalization in the Social Sphere
How Allosexuals Perceive and Interact With Asexuals
Prior to 2000, there was no research regarding perceptions of asexuality, and most assumed that asexual people did not face discrimination. A growing canon of work has emerged in the past decade showing that asexuals are routinely discriminated against and marginalized. The Development of The Attitude Towards Asexual Scale has laid the groundwork for a number of studies even within the past three years, and as time goes on this field will likely develop.Contact @asexualresearch on Twitter or [email protected] for articles that should be added, questions, or concerns!
Development and validation of the Attitudes Towards Asexuals (ATA) scale (Journal of Psychology And Sexuality)
“ Discomfort renting and hiring3
Discomfort renting to and hiring (MacInnis & Hodson, 2012) heterosexuals (α = .95), homosexuals (α = .96), bisexuals (α = .96) and asexuals (α = .98) was assessed using four items (e.g., ‘Indicate how comfortable you would be renting an apartment to people from each of these groups?’), rated on 11-point scales, with separate 4-item measures for each group. Scores were reverse-coded, with higher scores indicating greater discomfort rent- ing and hiring.”“ Interest in future contact (Husnu & Crisp, 2010) with heterosexuals (α = .92),
homosexuals (α = .94), bisexuals (α = .94) and asexuals (α = .91) were captured
using four items (e.g., ‘If given the chance, how interested are you in being friends
with someone from each of the following groups?’) rated on 8-point scales, with
separate 4-item measures for each group. Higher scores indicate greater future contact intentions.”
LGB within the T:
Sexual Orientation in the National Transgender Discrimination Survey and Implications for Public Policy
(This study examines sexual orientation and discrimination experienced by transgender people, an important step in analyzing the intersectionality of gender identity and sexual orientation.An important note about the data: Although only 264 asexual people responded, the researchers analyzed the data to make sure it was significant. The data with two asterisks are statistically significant, and those with one are statistically significant in the context of the complete study.)
Age of Participants (Interestingly, asexual respondents skewed older)
Familial Rejection
Public Accommodations And Incarceration
Housing
Racial and Ethnic Differences in Experiences of Discrimination in Accessing Social Services Among Transgender/Gender-Nonconforming People (Journal of Ethnic & Cultural Diversity in Social Work)
“The only difference on sexual orientation was that individuals who identified as asexual were more than twice as likely (OR = 2.37, 95% CI = [1.03, 5.46]) to have experienced discrimination at domestic violence shelters than heterosexual individuals.”
National LGBT Survey 2017 UK
The link above leads to the interactive data set. In the PDF library I have also included the analysis provided by researchers that the quotes arise from.
“Amongst cisgender respondents, gay and lesbian respondents were the most satisfied, compared to those with other sexual orientations, with an average rating of 6.88. Asexual and pansexual respondents were the least satisfied, with an average of 5.88 and 5.92 respectively (Figure 4.1).”“ Trans respondents had a lower life satisfaction, scoring it on average 5.40, than cisgender respondents, who scored it on average 6.67. Amongst trans respondents, trans men in particular were the least satisfied, scoring their life satisfaction on average 5.07 (Figure 4.2). Heterosexual trans respondents rated their life satisfaction the highest, scoring it on average 5.91, whilst asexual trans respondents rated it the lowest, scoring it on average 5.06 (Annex 4, Q152).”“Amongst cisgender respondents, gay and lesbian respondents were the most likely to score their comfort being LGBT in the UK as 4 or 5 out of 5 (63%), whilst asexual respondents were the least likely (49%) (Figure 4.4). Cisgender men were more likely to score their comfort as 4 or 5 out of 5 (63%) than cisgender women (54%) (Annex 4, Q11).”“ By sexual orientation, only 2% of gay and lesbian respondents had been open with none of their friends, whilst 12% of asexual respondents had been open with none of their friends (Figure 5.2). [greatest and least of the results]”“Openness with neighbours was generally low across sexual orientations, ranging from 39% of gay and lesbian respondents to 95% of asexual respondents having been open with none of their neighbours (Figure 5.6).”“ Broken down by sexual orientation, asexual respondents (89%), queer respondents (86%), and bisexual respondents (80%) were the most likely to avoid being open, compared to, for example, gay and lesbian respondents (66%) (Figure 5.11).““Fifty-eight per cent of asexual respondents said that they avoided being open about their sexual orientation at home, whereas only 14% of gay and lesbian respondents reported doing so. Some of this difference may reflect patterns of relationships and who lives with whom.”
On a scale of 1 to 5, how comfortable do you feel being an LGBT person in the UK? If you would prefer not to answer, please leave blank.
Overall, on a scale of 1 to 10, how satisfied are you with your life nowadays?
Do you ever avoid being open about your sexual orientation for fear of a negative reaction from others?
Where do you avoid being open about your sexual orientation for fear of a negative reaction from others?
In the past 12 months, did you experience any of the following from someone you lived with for any reason?
In the past 12 months, how many family members that you lived with, if any, were you open with about being LGBT?
In the past 12 months, how many people you lived with, if any, were you open with about being LGBT?
Think about the most serious incident in the past 12 months. Which of the following happened to you?
Who was the perpetrator(s) of this most serious incident?
Did you report this most serious incident?
Why did you not report this most serious incident to the police?
In the past 12 months, did you experience any of the following from someone you were not living with because you are LGBT or they thought you were LGBT? For example, from a friend, neighbour, family member you don't live, or a stranger. Please only include incidents that you haven't already told us about in this survey.
In the past 12 months, how many people in the following groups, if any, were you open with about being LGBT - Family members you were not living with?
In the past 12 months, how many people in the following groups, if any, were you open with about being LGBT - Friends you were not living with?
In the past 12 months, how many people in the following groups, if any, were you open with about being LGBT - Neighbours?
Think about the most serious incident in the past 12 months. Which of the following happened to you?
Who was the perpetrator(s) of this most serious incident?
Did you or anyone else report this most serious incident?
Why did you not report this most serious incident to the police?
Viewer Perceptions of and Attitudes Towards Asexuality in Response to Entertainment Media Representation (University of Twente)

"A Tukey post hoc test showed that the difference was between religious and non-religious participants on both the first (p = .001) and second (p < .001) measurement. On the second measurement, there was also a statistically significant difference between religious and ‘other’ participants (p = .045). The attitudes held by non- religious participants were therefore significantly more positive towards asexual individuals than the other groups in the respective measures.On the second question, ‘What is your opinion of the main character?’, 28.8% of respondents in the asexual condition, and 46.4% of participants in the unrelated condition, had a positive tone. There was a significant difference in tone between the conditions on the second open question [F(1,106) = 6.65, p = .011], with a mean score of 36.73 (SD = 36.78) with an average of 3.49% of the text reflecting positive emotions and 5.69% negative emotions in the asexual condition and 55.45 (SD = 38.52) with an average of 7.06% positive and 2.48% negative emotions in the unrelated condition. The difference between the asexual and unrelated conditions in positive emotions expressed was significant [F(1,106) = 4.33, p = .040], as was the difference between negative emotions [F(1,106 = 4.01, p = .048]. This shows that on the second open question, participants in the asexual condition had a less positive valence than the unrelated condition, and they also expressed overall less emotions. Of the emotions expressed, the asexual condition texts contained more negative than positive emotions, which was reversed in the unrelated condition.Although the greatest difference was expected to those that identified as “Conservative”, the fewer negative emotions expressed by “Liberals” compared to other groups was expected based on prior research. Aside from this, it was not expected that those who are “Non-political” have comparatively very low percentages of negative emotions in their texts, as previous studies have concluded that those who are more politically interested generally hold more positive attitudes to members of the LGBT community (Lee & Hicks, 2011; Norton & Herek, 2012; Whitley, 2001; Woodford et al., 2012). "
Judging an absence: Factors influencing attitudes towards asexuality (Trinity Western University Department of Psychology)
“Participants
The sample consisted of 1297 participants (48.6% women, 43.2% men, 6.4% nonbinary / other, 0.6% questioning) recruit- ed via sample-collecting and LGBTQ+ pages on social media sites. Gender was assessed through self-identification in an open-answer format. Some analyses were conducted with few- er cases due to missing data. The data were collected in Winter 2018 following IRB approval. Participants were informed that they were taking part in a study about perceptions of sexual minorities. All participants were required to be the age of ma- jority in their place of residence. Exclusion criteria included age below the age of majority, self-reported dishonesty, or a clear, consistent pattern of nonsensical responses. No compensa- tion was provided for participation in the study. Participants self-identified as non-LGBTQ+ (44.5%; n = 576), nonasexual LGBTQ+ (43.9%; n = 569), or asexual (11.0%; n = 143). Mean age was 25.9 (SD = 8.97; age range = 18–73). The sample was pri- marily North American (Canada, the United States, and Mexico; 72.0%; n = 935), with a majority speaking English as a first lan- guage (79.2%; n = 1028). 84.1% (n = 1091) of the sample report- ed at least some college or university or college education.
Measures
Participants completed baseline measures assessing demograph- ics, familiarity and attitudes towards asexual individuals, trait characteristics (openness, social dominance, right wing author- itarianism), behavioral intentions, and attitudes towards single people. This study uses a subset of measures taken from a larger study on attitudes and behaviors towards sexual minority groups.
Singlism
30 items were used to measure negative stereotyping of sin- gle persons (e.g., “It’s only natural for people to get married;” Pignotti & Abell, 2009). Higher scores indicate a more negative view of single persons (Cronbach’s α = 0.94 in the present sam- ple). This scale was included for the purpose of differentiating between antiasexual bias and bias against celibate or otherwise nonasexual single individuals.
Openness
Openness was measured using a 10-item subscale of the Big-Five Personality Inventory (e.g., “I see myself as someone who has an active imagination;” John, Donahue, & Kentle, 1991). Higher average scores indicated a more open personality; reliability in the present sample was Cronbach’s α = 0.72.
Social dominance orientation
The 16-item Social Dominance Orientation Scale was used to measure social dominance (Pratto, Sidanius, Stallworth, & Malle, 1994). A sample item is, “To get ahead in life, it is sometimes nec- essary to step on other groups.” Higher average scores represent stronger social dominance orientation. Reliability in the present sample was Cronbach’s α = 0.93.
Right wing authoritarianism
Zakrisson’s (2005) 15-item short form of the Right-Wing Authoritarianism scale was used to assess degree of authori- tarianism. A sample item is, “It would be best if newspapers were censored so that people would not be able to get hold of destructive and disgusting material.” Higher total scores repre- sent a stronger inclination towards right wing authoritarianism. Reliablity in the present sample was Cronbach’s α = 0.86.
Familiarity
Participants were asked to indicate whether they know anyone who is asexual. Those who indicated yes were then asked to rate from 1–7 the closeness of the relationships. We revised Hoffarth et al.’s (2016) definition of asexual to read: “people who have [little to] no sexual attraction to either sex (and never have).” The definition was revised to be in accordance with a more nu- anced understanding of asexuality that recognizes that some identities within asexuality may involve varying degrees of sex- ual attraction under particular conditions (Carrigan, 2011; Van Houdenhove et al., 2015a). Restricting asexuality to those who never experience sexual attraction under any condition could be a form of gatekeeping or an extension of asexual-exclusionist discourse (Donaldson, 2018; Hoins, 2017; Mosbergen, 2017).
Future contact and discrimination intentions
Following the lead of Hoffarth et al. (2016), interest in future contact (Husnu & Crisp, 2010) was modified in the present study to ask about the likelihood that an individual would have a con- versation, a friendship, or a dating relationship with an asexual person. Higher scores reflect a greater likelihood of future con- tact intentions with asexuals.
Discrimination intentions were assessed using a further 2 questions that asked about comfort with renting to and hiring asexuals. A sample item is, “How comfortable would you be with renting an apartment to someone who is asexual?”). Higher scores reflect a lower likelihood of discrimination intentions.
Attitudes towards asexual individuals
16 items were used to measure attitudes towards asexual individ- uals (Hoffarth et al., 2016; sample item: “People who identify as asexual probably just want to feel special or different.”). Higher average scores indicate a higher bias towards asexual individuals; reliability in the present sample was Cronbach’s α = 0.91.
RESULTS
Means and correlations for the key study variables are presented in Table 1. Nearly all respondents (91.52%; n = 1187) indicated at least moderate familiarity with the concept of asexuality. 46.03% (n = 597) know one or more asexual individuals. All study variables were associated with each other, which is unsurprising given the size of the study sample and the reliance on the litera- ture to select the study variables. However, most associations are either small or moderate, which minimizes concerns about col- linearity. Men were somewhat more than were persons of other genders to report negative attitudes (r = −0.31, p < .01). A small inverse association was found between openness and negative attitudes towards asexual individuals (r = −0.13, p < .01). Right wing authoritarianism was moderately associated with antiasex- ual bias, including negative attitudes (r = 0.46, p < .01), as was so- cial dominance orientation (r = 0.49, p < .01), as well as singlism (r = 0.53, p < .01).
We used multiple regression to test predictors of attitudes towards asexual individuals using a backward elimination pro- cedure (Table 2). A total of 9 independent variables were tested for inclusion in the model: age, gender, orientation, singlism, openness, social dominance orientation, right wing authoritar- ianism, knowing an asexual individual, and having a close rela- tionship with an asexual individual. Variables were kept in the model if p < 0.05. Results indicated that orientation (β = −0.15, p < .01), social dominance orientation (β = 0.33, p < .01), right wing authoritarianism (β = 0.02, p < .01), having a close rela- tionship with an asexual person (β = −0.03, p < .01), and sin- glism (β = 0.01, p < .01) explained 46.7% of the variance in atti- tudes towards asexual individuals (R2 = .47, F(5, 926) = 163.98, p < .01).
We also compared participants on attitudes towards asexual individuals based on three broad groups of self-reported orien- tation: non-LGBTQ+, nonasexual LGBTQ+, and asexual. While some participants indicated multiple overlapping identities, no participant was assigned to more than one group for the purpose of these analyses. Any indication of LGBTQ+ identity was sort- ed as LGBTQ+, unless the participant also reported an asexual identity (for example, participants who described themselves as asexual, demisexual, or aromantic). Heterosexual participants who did not indicate identification with either asexual or other LGBTQ+ identities were allocated to the non-LGBTQ+ group.
A one-way between subjects ANOVA comparing the effect of orientation (non-LGBTQ+, nonasexual LGBTQ+, and asexual) on attitudes found a statistically significant difference between orientations [F(2, 1063) = 48.87, p < .01]. Games-Howell post hoc comparisons showed that the mean scores for non-LGBTQ+ individuals (M = 2.13, SD = 1.31) were higher compared to non- asexual LGBTQ+ participants (M = 1.58, SD = 0.89) and asexual individuals (M = 1.36, SD = 0.35; M = 1.33). The differences be- tween the mean scores of nonasexual LGBTQ+ individuals and asexual individuals were not significant.”
Societal Challenge and Depression, Self-Esteem, and Self-Concept Clarity in Asexuals (University of Colorado Boulder)
“ About half of the asexuals (54%) chose three or below on the scale when asked how open they were with their families. Most stated that they hid their identity because their family was homophobic and would likely not react well to a nonstandard sexual orientation, or that past attempts to be open had received negative responses. Those who were open with their family often felt that they were misunderstood regardless of how open they were, and that their parents were displeased. One subject noted that when she ‘came out’ to her mother, she convinced her to keep it hidden from the rest of the family.
The majority (69.4%) of the asexuals who participated in the survey stated that they felt that their identity as an asexual had been challenged in the past. Those who felt they had had their identity challenged were most likely to have had it challenged by their friends, with family coming in second. Participants were least likely to have their identity challenged by an authority figure or their significant other, though approximately 14% of participants did have difficulty with their significant other’s views of their identity. “
UK National LGBT Survey 2020
"On average, respondents were less satisfied with their life nowadays than the general population, scoring it 6.5 out of 10, compared with 7.7 for the general UK population.9 Among cisgender respondents, gay/lesbian people had the highest scores (6.9) and pansexual or asexual people had the lowest scores (both 5.9). Trans people had low scores: trans men scored 5.1, trans women scored 5.5 and non-binary people scored 5.5.Average life satisfaction (out of 10)
Change between chart and table
UK Population 7.7
Gay/Lesbian 6.9
Bisexual 6.3
Pansexual 5.9
Asexual 5.9
Trans woman 5.5
Non-binary 5.5
Trans man 5.1UK Population
7.7
Gay/Lesbian
6.9
Bisexual
6.3
Pansexual
5.9
Asexual
5.9
Trans woman
5.5
Non-binary
5.5
Trans man
5.1Over half of the respondents (56%) felt comfortable being LGBT in the UK, rating their comfort as a 4 or 5 out of 5. Amongst cisgender respondents, gay and lesbian people were the most comfortable (63% comfortable) and asexual people were the least (49% comfortable). As with life satisfaction, trans people generally felt less comfortable. 37% of trans women, 34% of trans men and 38% of non-binary people felt comfortable being LGBT in the UK. Only 5% of all trans respondents aged under 25 said they felt very comfortable (scoring 5 out of 5), rising to 15% of those aged 55-64 and 31% of those aged 65+.
Safety
The existing evidence suggests that LGBT people are at greater risk than the general population of being victims of crime; Stonewall, for example, recently found in their YouGov survey that more than 25% of trans respondents who were in a relationship in the last year had been subject to domestic abuse.10 NIESR found that underreporting of hate crime is a particularly common issue. They also found that LGBT people can be unwilling to use relevant services for fear of homophobic, transphobic or biphobic responses from staff and service users or because they do not think the response will meet their needs. Data from the Crime Survey for England and Wales (CSEW) being published alongside this report for the first time reveal that gay, lesbian and bisexual people are more likely than heterosexual people to be victims of all CSEW crime.Openness about being LGBT
Over two thirds (68%) of all respondents with a minority sexual orientation said they had avoided holding hands in public with a same-sex partner for fear of a negative reaction from others. Similarly, 70% said they had avoided being open about their sexual orientation for fear of a negative reaction; this was higher for cisgender respondents who were asexual (89%), queer (86%), and bisexual (80%). The most common places where cisgender respondents had avoided being open about their sexual orientation were on public transport (65%) and in the workplace (56%). Some respondents described feeling safer moving to large cities with a significant LGBT population, like London, Brighton and Manchester."
Asexual and Non‐Asexual Respondents from a U.S. Population‐Based Study of Sexual Minorities (Archives of Sexual Behavior)
“Our hypothesis that asexuals would experience more stigma than non-asexuals was generally confirmed. Asexuals reported feeling more stigma than non-asexual men and women and more everyday discrimination than did non-asexual men. These results suggest that asexual identity is more stigmatized in society than LGB sexual minority identities. This supports prior research of MacInnis and Hodson (2012) who found that Canadian university students and online participants were more biased toward asexuals than toward LGB people. It also sup- ports the qualitative research of Gupta (2017) who interviewed 30 participants recruited from AVEN and other websites, and found that over half indicated that they had been stigmatized
or marginalized for being asexual. In Gupta’s study every par- ticipant mentioned at least one negative incident, such as get- ting medical or psychological explanations when they came out to family or friends, and feeling alienated from social events, classroom discussions about sex, conversations with friends, or media programs or advertising.“
Polish Asexualities: Catholic Religiosity and Asexual Online Activisms in Poland
“The report suggests that, much like other sexual minorities, asexuals are at a serious disadvantage in terms of mental health, social isolation, and social acceptance in Polish society (Świder and Winiewski 2017). For example, 22.9% of asexual people in the study indicated unfair treat- ment by the medical establishment, 21.9% mistreatment in their work- place, and 54.8% in their religious communities (Świder and Winiewski 2017, p. 48). Further, less than half of the asexual people in the study suggested that they would evaluate their life on positive terms, 68.2% have experienced social isolation, and 20.5% have frequent or very fre- quent suicidal thoughts (Świder and Winiewski 2017, pp. 54, 55, 57).“
Asexual Identity in a New Zealand National Sample: Demographics, Well-Being, and Health
(A study on people's perceptions of asexuals)
“In line with prior work on social avoidance, asexual men also had higher coldness, social avoidance, and non-assertive personality scores. Asexual women had higher scores on coldness, vindictiveness, social avoidance, non- assertiveness, and exploitable personality inventory indices. It was speculated that these differences might be partially due to the discrimination faced by asexual people, and living in a soci- ety that places a considerable emphasis on sex (see also Chasin, 2015; Scherrer, 2008).”
Societal Challenge and Depression, Self-Esteem and Self-Concept Clarity in Asexuals (University of Colorado Boulder)
"Asexuals were most open about their asexuality with their significant other and tended to keep it mostly hidden around their family, strangers, and authority figures. In the case of coworkers, many asexuals stated that it was not their business, though there were occasions where they felt pressured to state their sexuality. Most who hid their asexuality from authority figures did so from doctors and therapists for fear of their lack of sexual attraction being misconstrued as a symptom of an illness or mental disorder. Those who kept their asexuality hidden from the LGBT community stated that they did so because they had had unpleasant experiences with the community in regards to their asexuality in the past, while some stated that they were open with the LGBT community online but kept their asexuality hidden offline. Asexuals were asked how open they were about their sexuality on a scale of one to seven, with one being the most hidden and seven being the most open. About half of the asexuals (54%) chose three or below on the scale when asked how open they were with their families. Most stated that they hid their identity because their family was homophobic and would likely not react well to a nonstandard sexual orientation, or that past attempts to be open had received negative responses. Those who were open with their family often felt that they were misunderstood regardless of how open they were, and that their parents were displeased. One subject noted that when she ‘came out’ to her mother, she convinced her to keep it hidden from the rest of the family.
The majority (69.4%) of the asexuals who participated in the survey stated that they felt that their identity as an asexual had been challenged in the past. Those who felt they had had their identity challenged were most likely to have had it challenged by their friends, with family coming in second. Participants were least likely to have their identity challenged by an authority figure or their significant other, though approximately 14% of participants did have difficulty with their significant other’s views of their identity. The vast majority of challenges to asexuality that participants reported were phrases such as “you are a late bloomer” or “you have not met the right person.”The majority of the people who identified as asexual (69.4%) reported that they had their identity challenged in the past. It seems that the majority of asexuals, nearly 70%, have had their identity challenged or denied at some point and, judging by their comments, this has happened multiple times to many of them. The participants were the ones to decide whether they had been challenged or not, so it is possible that some people who may have had their identity challenged or denied by one definition did not by another, or vice versa. It is also possible that there are a number of people who have not had their identity denied because they keep their asexuality hidden from others for fear of rejection. Some who reported having their identity challenged may have not had it challenged directly; they may have seen something denying or discrediting asexuality on television or in a book. It may be worthwhile to see how this percentage compares to other sexualities and groups in the future. Asexuality as an orientation is a relatively new concept, and it is possible that things will change over time. LGB groups were hidden groups in the past, and LGB characters in the media started out as novel or stereotyped, but now LGB characters are relatively common, and tend to avoid stereotypical portrayals. Over the next decade or so we can probably expect to see asexuals and other non-standard sexual orientations, romantic orientations, and gender identities become more visible in the media, and in public discussions."
Asexuality: An Emergent Sexual Orientation (University of Saskatchewan)
"In response to the HHDRS items, participants reported experiencing a variety of
discriminatory behaviours, and hearing verbal insults on account of one’s asexual identity (15%), derogatory names being used to describe asexuals (13%), and anti-asexual remarks from family members (10%) emerged as the most frequently occurring events (see Table 1). These experiences, along with being treated unfairly by parents due to one’s asexual identity were pereceived as being stressful to varying degrees by 33%, 21%, 21%, and 23% of the sample, respectively. When examining the mean stress levels and ranges of stress evaluations for each experienced discriminatory episode (see Table 1), it is apparent that participants did not perceive the events to be overly stressful (possible range for these evaluations was 1-10, and the highest mean evaluation for any event obtained was 1.79, which participants perceived when verbally insulted due to their asexual identity). Moreover, participants’ total mean scale score (M = 23.14, SD = 9.90) on the HHDRS fell well below the scale midpoint of 84 and, thus, the sample experienced the types of discriminatory events included in the HHDRS relatively rarely.
Of interest, too, in the present study was obtaining an indication of the extent to which participants had disclosed their asexual identities to individuals of varying interpersonal closeness, as outlined on the OI. Percentages of participants who had disclosed their asexual orientation to each person/group of people were calculated, excluding those who responded with “not applicable” to any given item. Results indicate that most participants (85%) had disclosed their asexual orientation to at least one person, and a further 10% reported that they intend to disclose their asexual orientation in future. Participants’ responses were then divided into those who had disclosed their asexual identities and their identities were “definitely known” (i.e., responses on the OI of 5, 6, or 7 were given indicating that there was no uncertainty about participants’ disclosure) versus those who perceived to have disclosed their identity but the recipient of the information “probably knows” (i.e., responses on the OI of 1, 2, 3, or 4 were given indicating that a lack of certainty exists about the extent to which the person/group of people knows about a person’s identity). As seen in Table 2, of those participants who were certain that the individual/group in question definitely knows of their asexual identity, each had disclosed to his/her romantic partner, and over half of the applicable sample had disclosed totheir mental health care providers, old heterosexual, old non-heterosexual, and new non- heterosexual friends. Less than half of the applicable sample, however, had disclosed their identities to the remaining contacts listed on the OI.
Finally, the correlations between the HHDRS and the total OI, and the HHDRS and the OI subscales were calculated to determine the degree of association between the two measures. Scores on the HHDRS were significantly correlated with total OI scores, r(34) = .42, p = .01, scores on the religion subscale, r(35) = -.44, p = .01, and scores on the world subscale, r(34) = .50, p = .001. Scores on the HHDRS and the family OI subscale did not correlate significantly, r(35) = .30, p = .08. Overall, scores on the HHDRS and OI appear to be moderately associated.
DISCUSSION
To the authors’ knowledge, the present study is the first empirical investigation into
asexual individuals’ experiences of discrimination. In addition to measuring the types and sources of discrimination, a basic measure of the stress engendered by each experience from the participants’ perspectives was included. Further, the degree to which participants had disclosed their asexual orientation to various others also was investigated.
Responses to the OI indicate that a large majority of the sample had disclosed their asexual orientation to at least one person, and that almost the entire remainder of the sample was planning to do so in the future. This finding suggests that participants do not feel it necessary to completely hide their identity as asexual; however, the persons to whom they elect to disclose their identity was revealing. Specifically, only romantic partners, friends, and mental health care providers were those individuals to which over half of the sample had disclosed their identity as asexuals. Thus, although many participants had disclosed their asexual identity to at least one person, this aspect of their identity remains hidden from most of their proximal (e.g., family members) and distal (e.g., work peers and extended family) contacts. It is important to point out that the OI does not capture whether the disclosure of a participants’ asexual identity is deemed acceptable by others of varying interpersonal closeness. For example, although the OI measures whether one’s asexual orientation is openly discussed with one’s family members (e.g., brother/sisters), it does not measure whether the discourse is positive or negative in tone. Previous research has suggested that this discourse may, indeed, be highly negative and dismissive of asexuality and asexual relationships (Chasin, 2009; Scherrer, 2008, 2010). The inclusion of questions addressing the nature of the interactions with proximal and distal others would be useful.
With respect to the discrimination experienced by our sample, episodes of verbal harassment seem to be the most commonly cited. Specifically, insults, derogatory names, and anti-asexual remarks from family members due to one’s asexual identity were among the most frequent and stressful types of discrimination experienced. Based on these results, it seems that most participants had not experienced the types of blatant discrimination included in the HHDRS (e.g., physical violence or economic sanctions); however, the experiences reported suggest many perceive themselves to be living in environments in which their sexual identities are not accepted. The lack of perceived acceptance may fall under the rubric of subtle discriminatory behaviour (i.e., discrimination which is typified by acts that are derogative and hurtful, yet may or may not be ambiguous as to their prejudiced roots and intention to harm; Jewell, McCutcheon, Harriman, & Morrison, in press). For example, subtle discrimination may manifest itself in the form of gossip, use of anti-target language, and social distancing. Because the nature of subtle discrimination is not as well understood as its blatant counterpart (Jewell & Morrison, in press; Jewell et al., in press), the HHDRS is likely not as sensitive to the potential spectrum of subtle discriminatory behaviour experienced by asexual individuals. Some of the most frequently experienced events on the HHDRS, however, suggest that subtle discrimination may be an issue for the asexual community. For example, hearing anti-asexual remarks and being called derogatory names may be classified as subtle discrimination if the intent of the perpetrator was not to harm or ambiguous.
The family of origin seems to be a particular source of discrimination for asexual persons. Family members were conspicuously absent from the list of people to whom over half of the sample had disclosed their asexual identities. Indeed, participants reported disclosing their asexual identity less frequently to extended family members than to strangers. Again, the results of the OI do not indicate whether family members are accepting of participants’ asexual identities or not. However, the finding that family members were involved in two of the most frequent and stressful events on the HHDRS (i.e., unfair treatment by parents and anti-asexual remarks from family members) suggests that the familial environment can be negative for many asexual individuals.
The positive correlations between the HHDRS and the OI subscales suggest that participants who had disclosed their asexual orientation to others were also more likely to report experiencing the type of discrimination measured by the HHDRS. This result was anticipated because most of the HHDRS items refer specifically to discriminatory events that are precipitated by one’s asexual orientation. For example, to be rejected by a friend due to one’s asexual orientation, that friend would have to be aware that one is, in fact, asexual. One caveat to this conclusion was the negative correlation between the religion subscale and the HHDRS. Thus, participants who had disclosed their asexual orientation to members of their religious community reported fewer incidents of discrimination on the HHDRS. It may be that asexual individuals who are part of a religious community are more likely to be accepted by their acquaintances, or it may be that participants were more likely to disclose their asexual orientation to their religious community when they believed that it would accept their orientation. The present data, however, do not provide definitive conclusions regarding this relationship; thus, additional research designed to illuminate the nature of this association should be conducted."
“How do you Say ‘I’m Asexual’? It is even Difficult to Say”: The Construction of Asexual Masculinities in the Context of Sexual Imperative (From the Department of Philosophy, Sociology, Education & Applied Psychology, Università degli Studi di Padova, Padova, Italy)
“Overall, the results of our study are in line with earlier investigations about asexualities (DeLuzio Chasin, 2011; Gupta, 2015; Przybylo, 2011, 2012) and the link between nonsexuality and masculinity (Lopez Ruiz, 2015; Przybylo, 2014). The sexualization of interpersonal relationships appears to be a core dynamic in the cultural production of masculinity, as signaled by the precarious position occupied by asexual men in the domain of manhood. Specifically, the analysis of the interviews suggests that the delegitimation of asexual masculinities is performed in two ways: erasure and stigmatization.
Erasure relates to the scarce recognition of the disengagement from sexuality as a manifestation of a non- sexual identity. As previously emphasized by other authors (Gupta, 2017), our work points out that one of the major obstacles to the public visibility of asexuality is the difficult of finding definite and univocal behaviours to materialize one’s own asexual identification in the social field. Asexuality is largely, but not exclusively, narrated in terms of “lack” (see also DeLuzio Chasin, 2013; Przybylo, 2011) – of sexual desire, of sexual behaviours, of sexual attraction, of sexual pleasure – and the intelligibility of these manifestations of non-sexuality as an expression of asexuality is hindered by their reiterated misinterpretation as signs – or symptoms – of other sexual conditions (e.g. erectile dysfunction, shyness, latent homosexuality). In other words, asexuality is denied an independent ontological status in the field of masculinity as it is treated as a mere contingent epiphenomenon of other subordinated sexual masculinities.
The stigmatization refers instead to those situations in which asexuality, despite being regarded as an identification, is subjected in itself to emasculation, discrimination and other offensive behaviours. It is worthy of attention that the interviewees reported that their asexuality not only has been treated as more unacceptable than homosexuality, but also it has been denigrated even by men who identify in non- normative sexual orientations. This result seems to implicate that asexualities are placed in a perhaps moreprecarious and subordinated position in the field of manhood as compared to other non-normative sexual identities. This is in agreement with MacInnis and Hodson’s (2012) results about the higher rates of dehumanization towards asexual people and asexual men in particular.
Both in erasure and in stigmatization asexuality is sanctioned and delegitimated. Nonetheless, we believe that the process of erasure and misrecognition constitutes a specific form of violence (see Fine, Torre, Frost & Cabana, 2018) that goes beyond what has been identified as subordination in the scholarship about hegemonic masculinity. Indeed, in this case the link between masculinity and sexual desire is so intense that asexuality cannot occupy any position in manhood, not even a subordinate one: the existence of asexual masculinities is ignored or actively rejected. As a consequence, the behaviours and desires of asexual-identified men can enter in the field of intelligibility of masculinity only after being subjected to colonization by the sexual imperative, as they are redefined as yet another defective expression of the ubiquitous sexuality.
The relationship between asexual identities and the subordination of non-sexualities in the field of masculinity is far from linear. Even though asexual men are, as we discussed earlier, extensively targeted by emasculating stereotypes, we are persuaded that the asexual identification opens up a certain space for renegotiating the location of one’s own non-sexuality within or outside the available cultural definitions of masculinity. As maintained by Gupta (2017; see also Scherrer, 2008), the very existence of a term to materialize one’s own disengagement from sexuality as an identity provides a symbolic tool to create – in self-narratives, in social interactions and in public speech – a discursive space outside sexuality. Indeed, it being understood that asexuality is still far from being socially accepted, the shift from the almost complete inexpressibility of non-sexual subjectivities to the possibility to articulate the existence of asexuality envisages at least tensions and fractures in the sexual imperative and in the male sexual drive discourse. This process echoes other researchers’ conclusions about the disruption of heteronormativity produced by the emergence and visibility of sexual and gender non-normative identities (Bruce, 2013; Gamson, 1995; Malici, 2014, Primo, Zamperini, Testoni, 2019; Skeggs, 1999), and it is particularly cogent given the difficulties in making manifest one’s own non-sexuality. Claiming an asexual identity opens up a discursiveniche in the language of subjectivity from which it is possible to reject the dominant hypersexual connotation of masculinity. Nonetheless, the relationship between the stabilization of asexual identities and the social recognition of non-sexuality in general is controversial. Indeed, the constitution of a symbolic domain of asexuality is achieved also through the demarcation of a distinction between asexuality and other non-sexualities, as already pointed out by Flore (2013). Notably, in the case of masculinity the asexual identification can also enact a partial displacement of the emasculating stigma towards other non-sexual conditions, especially those who are commonly labelled as “sexual dysfunctions”.
To conclude, the findings of this study appear to provide further support to the growing belief that normative conceptions about the appropriate level of engagement with sexuality are at the core of the cultural organization of meaning associated with masculinity. In particular, we concur with previous works in this area in suggesting that asexual men inhabit an extremely precarious position in gender dynamics. The social rejection of non-sexual masculinities is so intense and widespread that they are not only subjected to subordination, but also to more radical forms of erasure and symbolic colonization. In addition, we believe that our inquiry provides important insights about the complex and multifaceted roles that the asexual identification plays in the constitution of non-sexual male subjectivities. As we emphasized, this relates not only to the renegotiation of the hegemonic position of heterosexual masculinities, but rather to a broader web of symbolic and material relationships that involves also non- normative sexualities and other non-sexual conditions. For this very reason, we suggest that a compelling topic for future research in the CSMM scholarships is the investigation of the heterogeneous interrelations among different subordinate locations in the field of manhood.”
Asexual People’s Experience with Microaggressions (City University of New York)
(This study is a 45-page document detailing the types, sources, and effects of microaggressions. For space restrictions, I have only included the conclusion.To read the complete study, check out the library.)“This study was done to discover if asexual people experience microaggressions, and if so, how the microaggressions manifested, who they came from, and what mental health effects they may have. Information from this study was also collected to inform further research, as well as increase competency for mental health care providers that have asexual clients. This study supports the proposition that asexual people do experience subtle discrimination known as microaggressions. The themes found were similar to the themes found in other research on LGBTQ identities (Nadal, 2011). The microaggressions came from the expected sources similar to other microaggression studies, such as family, friends, and the media. They did report some more overt forms of discrimination in the form of attempted sexual assault and nonconsensual touching that appeared to intersect with their gender identity; the participants all identified as women and women report a 1 in 5 rate of rape in the United States (NSVRC, 2015).
Discrimination has long been associated with negative mental health outcomes and distress, and microaggressions are starting to be associated with negative mental health outcomes as well (Nadal, 2011). It is important to know that asexual people are facing this form of discrimination and how it affects them so it can be combated and access to support and needed mental health care can be provided. Microaggressions also can come from healthcare providers and even mental health providers, as indicated in this study and others (Shelton & Delgado-Romero, 2011). Providers should be able to recognize the common microaggressions against asexual people so that they can avoid perpetuating microaggressions in the future and they can provide more competent and compassionate care. Microaggressions and discrimination have been previously shown to have negative effects on the mental health of LGB individuals, and the asexual participants in this study reported that microaggressions caused them increased anxiety, relationship stress, discomfort, and depression. Considering LGB people also report higher levels of mood disorders and personality disorders compared to heterosexual people, it is important to know what may be contributing to this, as they may be a population at a greater risk of negative mental health outcomes and in need of greater care (Yule, Brotto, & Gorzalka, 2013). They also may be seeking therapy more frequently because of their mental health and it is important to be culturally competent and aware of what asexual people face as a population. If health providers become aware of the experiences of asexual people, these individuals would be spared the need to explain their sexual orientation and freed from experiencing microaggressions in a health care setting where they need treatment.”
Intergroup bias toward “Group X”: Evidence of prejudice, dehumanization, avoidance, and discrimination against asexuals (Journal of Group Processes & Intergroup Relations)
Summary (written in Psychology Today article): In a recent investigation (MacInnis & Hodson, in press) we uncovered strikingly strong bias against asexuals in both university and community samples. Relative to heterosexuals, and even relative to homosexuals and bisexuals, heterosexuals: (a) expressed more negative attitudes toward asexuals (i.e., prejudice); (b) desired less contact with asexuals; and (c) were less willing to rent an apartment to (or hire) an asexual applicant (i.e., discrimination). Moreover, of all the sexual minority groups studied, asexuals were the most dehumanized (i.e., represented as “less human”). Intriguingly, heterosexuals dehumanized asexuals in two ways. Given their lack of sexual interest, widely considered a universal interest, it might not surprise you to learn that asexuals were characterized as “machine-like” (i.e., mechanistically dehumanized). But, oddly enough, asexuals were also seen as “animal-like” (i.e., animalistically dehumanized). Yes, asexuals were seen as relatively cold and emotionless and unrestrained, impulsive, and less sophisticated.-
Complete Findings: As predicted, attitudes toward heterosexuals (ingroup) were the most positive (see Table 1). Attitudes toward homosexuals, bisexuals, and asexuals were more negative than attitudes toward heterosexuals, revealing a sexual minority bias. Within sexual minorities, homosexuals were evaluated most positively , followed by bisexuals,
with asexuals being evaluated most negatively of all groups. Thus, not only are more negative atti- tudes leveled toward sexual minorities (vs. hetero- sexuals), but antiasexual prejudice is the most pronounced of all.Less favorable attitudes toward each sexual minority group were associated with increases in
RWA, SDO, ingroup (i.e., heterosexual) identifi- cation, or religious fundamentalism, as expected (see Table 2). Interestingly, relations between these prejudice correlates and attitudes toward asexuals are similar to relations between these variables and well-established sexual minority attitudes (i.e., attitudes toward homosexuals, bisexuals), despite the latter engaging in same- sex behavior whereas asexuals engage in no (or little) sexual activity. Prejudice-prone individuals, it seems, are biased against sexual minorities due to their deviant status rather than sexual actions perse.Attitudes toward sexual minorities (homosexuals, bisexuals, asexuals) were significantly and posi- tively intercorrelated, suggesting generalized sex- ual minority attitudes (see Table 2). That is, those liking (or disliking) homosexuals or bisexuals like- wise like (or dislike) asexuals. Furthermore, a confirmatory factor analysis supported a single factor of sexual minority prejudice: loadings .94 bisexual, .85 homosexual, .73 asexual.Trait-based dehumanization Uniquely human traits were perceived to apply most to heterosexu- als and were attributed less to homosexuals and bisexuals than heterosexuals (see Table 1). Asexu- als were attributed significantly lower uniquely human traits than any other sexual orientation group. Human nature traits were attributed signifi- cantly more to homosexuals than heterosexuals, bisexuals, and asexuals. Human nature traits were attributed significantly more to bisexuals than heterosexuals and asexuals, and heterosexuals were attributed significantly more human nature traits than asexuals. Thus, of the four sexual ori- entation groups, asexuals were perceived to be least “human” in terms of both uniquely human and human nature traits/characteristics.Emotion-based dehumanization A similar pat- tern emerged regarding perceived emotions expe- rienced by each group. Uniquely human emotions were perceived to be experienced most by homo- sexuals, followed by heterosexuals, and bisexuals; uniquely human emotions were perceived to be significantly least experienced by asexuals relative to all other targets. Human nature emotions were perceived to be most experienced by heterosexu- als and homosexuals, less by bisexuals (relative to heterosexuals and homosexuals), and experi- enced the least by asexuals relative to heterosexu- als, homosexuals, and bisexuals. As with trait-based dehumanization, asexuals were denied uniquely human and human nature emotions (see Table 1).Overall, participants indicated greater preference for future contact with heterosexuals relative to sexual minorities. Within sexual minority groups, contact with homosexuals was preferred over con- tact with bisexuals or asexuals (see Table 1). Again, thisdemonstratesevidenceofantisexualminority bias, and contact least desired with bisexuals and asexuals(equivalently).Ofparticularinteresttothe present investigation, contact with asexuals was desiredsignificantlylessthancontactwithhomo- sexuals, a frequently studied prejudice target group.
Participants were most willing to rent to hetero- sexuals relative to sexual minorities. Following heterosexuals, participants were most willing to rent to homosexuals or asexuals, and least to bisexuals. The same pattern was observed with regard to hiring decisions (see Table 1). Overall, participants intended to discriminate against sex- ual minorities (including asexuals), with most bias directed toward bisexuals.Importantly, attitudes toward asexuals do not simply reflect negative biases toward single peo- ple. In fact, attitudes toward asexuals were not significantly related to singlism (see Table 2). Moreover, relations between RWA, SDO, ingroup identification, or religious fundamentalism and asexual attitudes remain relatively unchanged after statistically controlling for singlism (partial correlations equal −.41, −.31, −.29, and −.25, ps < .001, respectively).Empirically, very little is known about asexuality relative to other sexual orientations, and no research has addressed whether asexuals are tar- gets of bias at the group level. Addressing this lat- ter question for the first time, our analysis suggests that antiasexual prejudice is indeed a sexual minor- ity prejudice, correlating positively with attitudes toward homosexuals and bisexuals. Relative to the heterosexual ingroup, we find compelling evidence of antisexual minority prejudice, with this newly identified bias being particularly extreme. Strikingly, on many key measures (particularly intergroup evaluations, dehumanization, and for the most part, contact intentions), we find significantly more bias against asexuals than other sexual minorities, and discrimination intentions matching that against homosexuals. Overall, we find clear evi- dence of a previously unidentified and strong sex- ual minority prejudice: antiasexual bias.
In keeping with this bias being intergroup in nature, those higher (vs. lower) in RWA or SDO expressed particularly strong dislike of asexuals, as they typically do for deviant and low-status groups. In keeping with social identity theory, stronger heterosexual identification was also associated with greater asexual prejudice. This relation between heterosexual identification and favorable evaluations of asexual people became smaller when statistically controlling for RWA and SDO, but remained significant (rp = −.19, p = .022). Overall, negativity toward asexuals is marked by an ideological flavor that is clearly intergroup in nature, not a simple indifference toward a nonnormative other. Importantly, although those higher in SDO or RWA expressed greater singlism, their dislike of asexuals was not explained by singlism. Antiasexual bias is a type of sexual minority prejudice distinct from related constructs and rooted in ideological opposition to deviant sexuality (not merely those adopting independent or single lifestyles). That is, antia- sexual bias is not merely singlism.
Those higher (vs. lower) in religious funda- mentalism also demonstrated less favorable atti- tudes toward asexual people, despite asexuals being disinterested in sexual relations, a relation that remains after statistically controlling for SDO (rp = −.19, p = .019). Upon statistically control- ling for RWA however (rp = .05, p = .548), or both RWA and SDO (rp = .03, p = .698), this relation- ship reduces to nonsignificance. This latter find- ing is unsurprising, given that few variables predict prejudice above and beyond RWA and SDO (see Altemeyer, 1998). Further, strong correlations typically exist between RWA and religious funda- mentalism (r = .67 in the current study), leading Altemeyer and Hunsberger (2004) to consider religious fundamentalism a “religious manifesta- tion” of RWA. Thus, while evaluations of asexu- als are more negative among prejudice-prone individuals, asexual prejudice does not have a unique religious component, but rather reflects concerns with status quo and group dominance.
Our dehumanization results are particularly compelling. Asexuals (relative to heterosexuals) were dehumanized with regard to both dimen- sions (represented as animalistic, and particularly as machine-like), regardless of whether these assess- ments were based on traits (i.e., characteristics) or emotions (i.e., sensation capability). Generally speaking, asexual dehumanization was greater than that characterizing other sexual minorities, showcasing this bias as serious and extreme. Sexuality appears to be perceived as a key compo- nent of humanness. The dehumanization meas- ures employed did not explicitly reference sexuality, yet asexuals were strongly biased against on these measures. Thus, characteristics/emo- tions representing humanness are clearly inter- twined with sexuality and/or sexual desire.
The researchers then replicated the study with a new population.
Replicating Study 1, a sexual minority bias was demonstrated whereby attitudes toward heterosex- uals were the most positive, followed by attitudes toward homosexuals, bisexuals, and asexuals. Within sexual minorities, homosexuals and bisexu- als were evaluated equivalently, with asexuals evalu- ated more negatively than both homosexuals and bisexuals (see Table 3). Again, the pattern of antia- sexual prejudice, relative to the heterosexual ingroup and even relative to other sexual minorities was uncovered. Importantly, this general pattern of differential evaluation of sexual orientation groups matches that of Study 1, even though atti- tudes toward each group are more positive in the online (vs. student) sample (ps < .003).As in Study 1, less favorable attitudes toward sex- ual minority groups were associated with increases in RWA, SDO, heterosexual identification, or reli- gious fundamentalism. In one exception, attitudes toward asexuals were not significantly correlated with religious fundamentalism (see Table 4). Overall, associations between attitudes and RWA, SDO, and heterosexual identification corroborate our findings from Study 1: prejudice-prone indi- viduals are more biased toward asexuals, as they are toward other sexual minorities (note that, unlike Study 1, the relation between heterosexual identification and bias toward asexuals reduces to nonsignificance when statistically controlling for RWA and SDO, consistent with the notion that bias against asexuals is about conventionality, tra- ditionalism, and group dominance).As in Study 1, attitudes toward sexual minorities were positively intercorrelated (see Table 4) with a confirmatory factor analysis supporting a single factor of sexual minority prejudice: loadings .97
6 bisexual, .89 homosexual, .76 asexual .Uniquely human
traits were perceived to apply most to heterosexuals and homosexuals, and attributed less to bisexuals and asexuals than heterosexuals (see Table 3). Human nature traits were perceived to apply equiva- lently to heterosexuals, homosexuals, and bisexuals, with asexuals attributed significantly lower human nature traits than each of the other groups. Thus, evidence of antiasexual bias was again evident.Both uniquely human and human nature emotions were per- ceived to be experienced equivalently by hetero- sexuals, homosexuals, and bisexuals, and experienced significantly less by asexuals relative to each of the other groups. Again, asexuals were relatively denied uniquely human and human nature emotions (see Table 3).Confirming Study 1, heterosexuals indicated prefer- ence for future contact with heterosexuals relative to
sexual minorities. Desired future contact with homosexuals and bisexuals were equivalent, and contact with asexuals was even less desired than contact with homosexuals (see Table 3).A sexual minority bias was evident, whereby par- ticipants were most willing to rent to and/or hire heterosexuals relative to homosexuals, bisexuals, or asexuals (see Table 3).In Study 2, less favorable attitudes toward asexu- als were related to greater singlism (r = −.22), but not so much as to indicate strong conceptual overlap (see Table 4). Furthermore, relations between RWA, SDO, or ingroup identification and favorable attitudes toward asexual people remained significant after statistically controlling for singlism (partial correlations equal −.30, −.26, −.22, and ps < .03, respectively). These findings further corroborate the proposition that biases against asexuals concern their sexual deviancy rather than simple biases against those who are relatively independent and not in committed sex- ual relationships.As noted previously, bias against asexuals might reflect a bias against a relatively unfamil- iar sexual minority, rather than asexuality per se. This potential explanation, however, is not supported. Heterosexuals were not surprisingly the most familiar sexual orientation group (M = 8.90). Homosexuals (M = 8.51) were less familiar than heterosexuals, followed by bisex- uals (M = 7.92) (ps < .001). Asexuals (M = 5.80) were less familiar than heterosexuals, homosexuals, and bisexuals (ps < .001). As expected, sapiosexuals (M = 2.67) were deemed significantly less familiar than heterosexuals, homosexuals, bisexuals, and most critically, asexuals (ps < .001).
Although asexuals were not the least familiar sexual minority target, they were nevertheless the most negatively evaluated. That is, attitudes toward asexuals were significantly more nega- tive than attitudes toward sapiosexuals (M = 6.81), t(100) = 2.24, p = .027. If lack of famili- arity were solely responsible for the pattern of group evaluations obtained (see Tables 1 and 3), sapiosexuals would be the most negatively eval- uatedgroup.Infurtherevidencethatfamiliarity per se does not explain dislike of asexuals, rela- tions between RWA, SDO, or ingroup identifi- cation with asexual evaluations were relatively unchanged after statistically controlling for familiarity with asexuals (partial correlations equal −.36, −.31, −.24, and ps < .02, respec- tively). Prejudice-prone persons, therefore, were not more prejudiced toward asexuals as a result of mere unfamiliarity.Employing an online community sample, the results of Study 2 largely confirm those from the university sample examined in Study 1. Asexuals were evaluated negatively relative to both hetero- sexuals and other sexual minorities, with order effects not explaining this pattern given the rand- omized order of evaluations. Notably, asexuals were evaluated more negatively than a very unfa- miliar sexual minority comparison group, sapio- sexuals. The group lacking sexual desire, rather than the least familiar group, was the target of the most negative attitudes. Again, we provide evi- dence that antiasexual bias is a form of sexual minority prejudice, that those prone to prejudice are more prone to antiasexual bias, and that asex- uals are targets of dehumanization, avoidance, and discrimination intentions. Further, we dem- onstrate that bias toward asexuals is either equiva- lent to, or even more extreme, than bias toward homosexuals and bisexuals.
Although these results largely corroborate Study 1 some interesting differences emerged. First, mean evaluations of each group were noticeably more positive in Study 2. Interestingly, university students were more negative toward homosexuals, bisexuals, and asexuals than the population in general. This might come as a sur- prise given university students’ reported tendency toward liberalism and lower prejudices toward most other social targets (Henry, 2008). This finding suggests that university-aged students strongly value heteronormative sex, viewing sex- ual minorities, especially those preferring no sex at all, as deficient. Second, although asexuals were dehumanized on both dimensions (uniquely human and human nature) by the overall sample, sex differences emerged, whereby men repre- sented asexuals as animalistic more consistently than did women (see Endnote 5). There was a strong overall tendency however, as in Study 1, for asexuals to be viewed by both men and women as more machine-like than heterosexuals, homosexuals, or bisexuals. Overall, asexuals are clear targets of bias by heterosexuals.
Discussion of Findings In Both Studies
We have established consistently that asexuals are evalu- ated negatively (not due to a simple lack of famili- arity). Asexuals’ status as a highly atypical and “deficient” (Herek, 2010) sexual minority group seems to be a more likely source of this prejudice. We have established various forms of antiasexual bias (including dehumanization) relative to heter- osexuals and, in some cases, other sexual minority groups. Taken together, Studies 1 and 2 confirm the existence of antiasexual bias, in university and community samples, respectively.
Our findings are in keeping with Herek’s (2010) “differences as deficits” model of sexual orientation, where sexual minorities deviating from the norm are considered substandard and deserving of negativity by the majority. This model is gradually becoming less applicable to homosexuals and bisexuals with changes in soci- etal norms (Herek, 2010), consistent with our findings that homosexuals (and in some cases bisexuals) were viewed as equally or more human than the heterosexual ingroup . However, we
posit that asexuals fit well within the “differences as deficits” framework. Asexuals are the sexual minority that is most clearly considered “defi- cient” by heterosexuals. In keeping with this interpretation, themes relevant to maintaining the status quo and group dominance (RWA and SDO, respectively) proved consistently important in predicting antiasexual attitudes, whereas con- cerns with positive ingroup identity and religious fundamentalism were less uniquely important.
Although antiasexual bias is a clear compo- nent of sexual minority prejudice, it is also unique in that it was repeatedly stronger than bias toward other sexual minorities. Most disturbingly, asexu- als are viewed as less human, especially lacking in
terms of human nature. This confirms that sex- ual desire is considered a key component of human nature, and those lacking it are viewed as relatively deficient, less human, and disliked. It appears that asexuals do not “fit” the typical defi- nition of human and as such are viewed as less human or even nonhuman, rendering them an extreme sexual orientation outgroup and very strong targets of bias. Future research can address the mechanisms underlying this tendency.
“And Now I’m Just Different, but There’s Nothing Actually Wrong With Me”: Asexual Marginalization and Resistance (Study Published in the Journal of Homosexuality)
"A number of scholars studying asexuality have argued that although Western society is certainly “sex negative” in some ways, Western society also systematically privileges sexual identifications, desires, and activities while marginalizing different forms of non- sexuality, to the detriment of asexually identified individuals (for example, Chasin, 2013; Emens, 2014; Gupta, 2015a). According to some scholars, asexual commu- nity formation poses a challenge to this society-wide system of “compulsory sexuality” or “sex-normativity,” calling into question deeply held assumptions about sexuality and relationality (Chasin, 2013).A number of studies have explored one or more of the negative impacts of contemporary sexual norms on the lives of asexually identified individuals. According to this scholarship, asexually identified individuals can face pathologization (Foster & Scherrer, 2014; Robbins, Low, & Query, 2015), difficulties in relationships and social situations (Carrigan, 2011), and disbelief or denial of their asexual self-identification (MacNeela & Murphy, 2014).In response to a direct question about whether they had ever felt stigmatized or marginalized as a result of their asexual identity, more than one half of the interviewees answered “yes,” more than one quarter answered “maybe” or “in some ways yes, in some ways no,” and around 20% answered “no.” In addition, all the interviewees described at least one negative experience attributable to compulsory sexuality. Here I offer a typology of these negative impacts of compulsory sexuality: pathologization, isolation, unwanted sex and relationship conflict, and the denial of epistemic authority. It is important to emphasize that what follows should not be taken as direct evidence of marginalization, stigma, or discrimination but as the interviewees’ interpretations of and narratives about particular life experiences.Isolation and invisibility
When asked about experiences of stigma or marginalization or if they saw any
negative aspects to identifying as asexual, at least two thirds of interviewees
reported occasionally feeling isolated or alienated from others or from society as
a result of the stigmatization or invisibility of nonsexuality. For example, Hannah talked about avoiding restaurants, bars, and clubs to avoid feeling isolated: “I think that a lot of social activities are like that, a lot of people think the goal is to hook up...So I sort of don’t want to participate in these sorts of things.” Anne, a current undergraduate majoring in psychology, described feeling isolated during a classroom discussion about sex: “It’s sort of a lonely feeling...everyone was like laughing and so forth, and I was kind of like ‘Ha-ha-ha, I don’t really get it,’ you know?” Sharon, age 49, described being bullied as a child, which she attributed to her weight and social awkwardness and to her lack of interest in dating or sex. She said, “I know my general social awkwardness, especially then, was a big part of what made me a target for them, but I also think that the asexuality played a significant part as well. I didn’t react to those boys the way they wanted me to. I had no sexual interest in them, and didn’t know how to fake it.”
At least 12 interviewees described feeling left out when their friends or peers talked about sex. For example, Lilly, 19, stated, “There would be a sleepover and people would be like, ‘Let’s play truth or dare.’ And almost all the questions are like, ‘Oh, who do you like? Have you ever kissed a guy? Who do you have a crush on?’ And I’d just be sitting there, like, ‘I don’t have a crush on anyone.’ ... And usually they’re like, ‘Oh, you’re boring.’”
At least eight interviewees described feeling isolated as a result of what they perceived as the overwhelming sexualization of the media and advertising. Mark, 25, said, “And now there’s sex everywhere...Also, sex sells on television, commercials, television shows...It’s just—I feel like it’s everywhere.” At least seven interviewees reported feeling isolated because asexuality is not represented in the media. Lilly said, “And so definitely the main thing that we face is erasure...the number of [asexual] characters in books and movies and TV who openly identify as asexual is two...it’s hard to figure stuff out just because there’s no examples.”Denial of epistemic authority
Lastly, in response to a question about how others had responded to their (a) sexuality, almost two thirds of interviewees reported at least one experience where they had been denied epistemic authority in regard to their own
sexuality. In other words, according to these interviewees, they had been met with the reaction that they could not know that they were asexual—they were told that they could be late bloomers, they had not met the right person yet, or they were repressing their sexual desires. About this Hannah said, “They insist that you essentially are not mentally competent to make your own decisions about yourself, which is really insulting to imply. You’ve met them for five minutes and they automatically know that you can’t make decisions by your- self. Like that’s really rude.” This was a response that interviewees reported encountering even in some LGBT communities. Eleanor, 50, said, “Nobody will just say, ‘Cool, you’re asexual.’ ... Even among gays and lesbians—that’s the one that always freaks me out—that gay and lesbian people can’t under- stand since they have a unique sexuality. But I guess they feel like everyone should have a sex, want to have sex, be attracted sexually to people.” On the other hand, it is important to note that at least 17 interviewees also described an instance in which they received a supportive response upon coming out.
A mystery wrapped in an enigma – asexuality: a virtual discussion (Interview with prominent researchers in asexuality)
"How is the negativity directed toward asexual individuals similar to/different from the negativity directed at other sexual minorities (e.g., gay men, lesbian women, etc.)?
I imagine that the similarities in the negativity experienced would revolve around the ‘magic cure.’ How many times has a lesbian woman been told ‘all you need is a good fuck by a real man?’ As if a lesbian woman is only interested in women because she hasn’t ‘met the right man.’ I have personally been told that if I just slept with a woman I would ‘absolutely fuckin’ love it’ and I would be ‘normal.’ I would imagine the same would be true for asexual individuals, being told that all they need is sex with someone (of the opposite sex of course) to ‘cure’ them and make them ‘normal.’
– BishopWe need to remember that many asexual individuals also identify as gay, lesbian, bisexual, transgender, and/or queer, and thus may face the same types of negativity directed at other LGBTQ individuals. My general impression from the U.S. context is that the negativity directed at asexual individuals is similar in some ways to the negativity directed at other sexual (and gender) minorities: asexual individuals, like other sexual minorities, may be perceived as mentally or physically ill, asexual individuals may feel alienated in social settings organized to facilitate heterosexual coupling, and asexual individuals may be denied legal and/or social recognition of their most important relationships. On the other hand, to a perhaps greater extent than other sexual minorities, asexual individuals are often denied ‘epistemic authority’ in regards to their own (a)sexuality. In other words, asexual individuals may be met with the reaction that they can’t really know that they are asexual – maybe they haven’t met the right person yet, maybe they are ‘late bloomers,’ maybe they are unconsciously repressing their sexual desires, maybe there is a physical cause of their asexuality that simply hasn’t been found yet. It is also my impression that asexual individuals in the U.S. (who do not also identify as LGBTQ) do not seem to be widely subjected to some of the more virulent hostility directed at other sexual and gender minorities, such physical battering and employment discrimination.
– GuptaWhat directions do you expect asexuality research to take over the next decade?
I hope that at the very least future research will not focus on how to ‘fix’ asexual individuals and will instead focus on them as people and the struggles they face. I realize this is unlikely to happen as there will be labs out there funded by religious groups or other ‘crusaders’ who want to ‘help’ asexual individuals. But still, a guy can dream.
– Bishop"
Freedom and foreclosure: Intimate consequences for asexual identities (Journal of Family Relationships And Societies)
“These participants thought of themselves as being inherently different; as Lisa poignantly says here,“not even a proper human being”.This shows the two ways in which identity can occur via dissociation from others (Skeggs, 2005). First, one’s self-identity can shape what we think we can or cannot do and therefore the strategies we adopt. In this case, the lack of experience of sexual intimacy is foundational to Deena’s account – which she feels means that she cannot fully participate in her friendships. Consequently, Deena practiced faking with her female friends – she internalised the cultural script and, much like Immy, developed a way of ‘passing’ to hide what she believed was the discreditable stigma of her lack of sexual experience. She used this ‘cover story’ as a strategy of information control for the purposes of dramaturgical self-presentation (Goffman, 1959, 1963). Second, interactions and relations affect self-identity: being unable to relate to others about something that is so important to her made Lisa feel excluded and alienated.This inevitably affected her sense of self and reinforced the feelings of difference; of ‘not being a proper human being’.Therefore, here we see the ways in which the cultural ‘sexual assumption’(Carrigan,2012) can lead to forms of exclusion for those who do not fit within it.“
Mental Health Disparities by Identity Among Gender and Sexual Minorities (University of Minnesota)
"In addition, victims of LGBTQIA2S+ hate crimes are more likely to experience indifference and abuse from law enforcement when attempting to report the crime, another example of structural stigma which could compound the stress of being victimized in the first place (Hein & Scharer, 2012).
Asexual, bisexual, and trans people experience more marginalization in society in general, and although this marginalization extends to psychological research, the research that has been done shows that mental health disparities are more severe for these particular groups.
When comparing the different types of negative attitudes and bias of heterosexuals toward different sexual minority identities, it was found that regardless of whether bias was based on “right wing authoritarianism,” (bias based on ideology) or “social dominance orientation,” (bias based on cultural norms) heterosexuals had most negative attitudes and bias toward asexuals, followed by bisexuals, with homosexuals as the sexual minority receiving the least bias and negativity (MacInnis & Hodson, 2012). This demonstrates that there is more individual bias toward the more marginalized identities in order of marginalization, so bisexuals experience more negativity and bias directed toward them than gay or lesbian people, and asexuals experience even more. It is possible that this bias is directed toward identities perceived as more “deviant”: asexuals may be more deviant because they do not conform to the social expectation that everyone is interested in sex (MacInnis & Hodson, 2012). It was also found that asexuals were seen in dehumanizing terms by the participants, who labeled them as lacking both “uniquely human” and “human nature” qualities, meaning they were seen as inhuman in both animalistic and machine-like ways (Macinnis & Hodson, 2012). These negative attitudes contribute to interpersonal stigma, a minority stressor."
Passing When Asexual: Methods for Appearing Straight (McKendree University)
“ The research indicated that coming out occurs in liberal spaces and passing occurs in conservative spaces. The findings showed that all but one participant both passed and are out to some extent. The great majority of the participants were out to friends at college, a typically liberal space. This is revealed by the fact that Karen reported that she came out to her college friends because she knew that they would accept her. Emily and Elayne reported similar experiences and reasons for coming out. Conversely, participants showed tendencies to pass at home and in church, both traditionally conservative areas. Families were reported as being less understanding, or at least less knowledgeable, than the environment at school (Emily, Toni, Karen, Sam Interviews). The final analysis of the research indicates a strong sentiment that the information that is available for people new to the asexual community is largely inadequate and difficult to find. This reveals that there is a legitimate need for more widely available information about asexuality, not only for those who are beginning to identify but also for those who do identify as well as families that need to understand. Passing is a perceived necessity that has long been associated with sexual deviance, and minority status (Wallqvist and Lindblom 2015). Understanding how and why asexual people pass is a crucial facet of understanding asexuality as a whole.”
Stories About Asexuality: A Qualitative Study on Asexual Women (Journal of Sex & Maritial Therapy)
"Given that they did not have a name or label to describe how they felt, 4 women thought there must be something wrong with them.With the exception of 2 women, all participants have come out to others, at least partially: they have told other people that they are asexual. Jessica, 30 years old and single, described how she felt forced to come out so she could have a normal relationship with her mother.
Ihadtocomeout,becausenowuhm... nowIcanhaveanormalconversationwithmymother,until that time our conversation only regarded relationships, and then I got angry, and then she got angry and we were both angry. Eventually, all we did was fighting, and that’s why I have decided to come out.
(Jessica, 30 years old, single)
Other women did not feel this pressure but decided to tell people about their asexuality because they had accepted their own identity and wanted to share that with others, given that it is a part of who they are.
It was nice to talk to people about it and to hear: maybe that’s just how it is. Yeah, someone agreeing with me on that, that was really nice.
(Mia, 31 years old, single)
When telling people about their asexuality, the participants in our study received mixed reactions. Five women received negative reactions ranging from not understanding, not believing in the existence of asexuality, to unwanted advice about the necessity to change their asexuality. Emily illustrated these negative reactions prototypically:
Disbelief, like: it’s just a phase, it will change one day, you just haven’t met the right person yet, you just haven’t been truly in love yet. Things like that.
(Emily, 20 years old, in a relationship)While 5 women stated that being asexual did not have a major effect on their currently daily life, 4 participants nevertheless indicated changes since they realized they are asexual. For example, 26-year-old and single Chloe described how it has changed her social life:
I’ve noticed that I less often feel like going out with friends, for instance because then you’re in that situation again and I don’t want that. [ . . . ] While before, I used to love it, going out dancing, but then it didn’ t have that connotation yet. [... ] Now, when I go out and I meet men, I try to stay as neutral as possible.
(Chloe, 26 years old, single)The support of an online community might especially be important given that recent evidence showed that asexual individuals may be viewed more negatively than other sexual minorities (MacInnis & Hodson, 2012). This was also somewhat reflected in the negative and dismissive reactions some of our participants experienced when they came out. Scherrer (2008) and Bogaert (2012) noted that the process of identity development in asexual persons shows similarities with the processes of developing a lesbian, gay, or bisexual identity. The possible parallels in sexual identity development between lesbian, gay, and bisexual individuals and asexual individuals could be informative for clinicians when asexual individuals would consult them. After all, this would imply that asexual persons experience struggles and (minority) stress similar to those of lesbian, gay, and bisexual individuals and that when asexual persons would seek clinical counseling, attention should also be paid to these topics, apart from working toward acceptance of the asexual identity."
“I have a lot of feelings, just none in the genitalia region”: A grounded theory of asexual college students’ identity journeys (Journal of College Student Development)
“This research also brings awareness to pervasive allonormativity and the negative influences asexual invisibility, invalidation, and erasure have in the lives of asexual students. Max provided an important summative comment, “Being invisible isn’t a privilege, and it’s not [pause] I don’t know how to describe it because I feel like it’s too obvious for words in a lot of ways.” Max’s words underscore the narratives of participants who collectively felt they were broken, obstacles to their development, and experiences of oppression fueled by the invisibility of asexuality. These findings align with Robbins et al., (2016) perceptions about invisibility including the unique role of the internet in discovering asexuality and students’ likelihood to pathologize their lack of attraction before gaining awareness of asexuality.
In a 2015 online survey of asexual college students, 70% of participants identified increased awareness of asexuality as a top priority for improving higher education for asexual students (Author, 2015). The findings from this study further illuminate the imperative of asexual visibility. Increased visibility represents a pivotal tool for supporting asexual students in finding and understanding their identities. If students knew asexuality existed, perhaps their journeys gaining awareness of asexuality, could include more personal authority and less feelings of uncertainty and inadequacy. This is not to suggest that visibility is all that institutions should do to support asexual students; rather, acknowledging that asexual students exist and creating awareness represents a necessary foundation to begin deconstructing allonormativity and supporting identity development of asexual students.
In students’ expatiation, the salience of their asexual identities as well as their other identities also influenced their processes and experiences of asexual identity development. The study findings clearly indicate the inextricable connection between asexuality, students’ multiple identities, and the multiple oppressive societal influences. Across the entire ASE model, students’ multiple minoritized identities influenced their identity journey from how they found asexuality, the salience of their asexuality, and how they integrated asexuality within their lives. Students with multiple minoritized identities often engaged in more expansive identity exploration as they tried to put the pieces together inclusive of all of their identities.
Students with multiple minoritized identities discussed ways oppression of their multiple identities, in conjunction with their asexuality, created cumulative marginalization. Of particular note, the experiences of intersectional invisibility described by the Students of Color emphasize lasting effects of whiteness associated with asexuality. The participants in this study did not specifically mention the overt omission of race from AVEN or the historic foundations of asexual as a racialized term; rather, they acknowledged the broad invisibility of asexual People of Color in any contexts they had discovered. Gender and ability stereotypes influenced students’ though the entire model. The experiences of asexual students with multiple minoritized identities underscores the continued importance of not examining students’ identity development in fragmented or isolated ways.
The findings integrating students’ multiple identities align with the findings from Foster et al. (2019) study of asexual WOC. They similarly identified participants’ feelings of isolation, particularly in struggling to find asexual Communities of Color. Within the domain of identity development processes, the ASE model supports several of their findings including experiences of making sense of differences, negotiating personal definitions of asexuality, and acceptance of asexual identity. These similarities highlight areas for continued research centering asexual college Students of Color.”
“Maybe all these random experiences form a cohesive picture”: towards a grounded theory of asexual college students’ identity development (a book-length exploration into the effects of asexuality on twelve college students from The University of Iowa)
“This study explored the experiences of 12 college students as they reflected on their journeys to understand their sexual identities. Each of the students identifies as asexual. In other words, they have little to no sexual attraction to people of any gender. Distinct from celibacy (which is a choice to refrain from sexual behavior), the students described feeling a sense of difference from peers and family during their adolescence. Using an interview-based method, students shared about memorable experiences related to their asexual identity.
From the participants’ experiences, a theory emerged as a potential representation of asexual college student identity development, the Asexual Student Expatiation Model (ASE). The ASE model demonstrates the complexity and non-linearity of the students’ experiences within societal structures that invalidate asexuality. Within the model, students engaged in processes of assimilating, searching for meaning, seeing themselves as asexual, situating in society, internalizing negativity, and experiencing wholeness. The students’ stories detail their unique and individual experiences and paths navigating gaining awareness, identifying, and reconciling asexuality in their lives with their other identities.
The study informs future research, theory, and college student affairs professionals. Recent estimates suggest that more than five percent of college students may identify as asexual. Despite the suggested prevalence, this is the first study of asexual college students that uses their narratives as the foundation for exploration.“
Coming To An Asexual Identity: Negotiating Identity, Negotiating Desire (from Sexualities: Sage Journals)
"As suggested throughout, there are myriad connections between asexuality and other sexual minorities. First, asexuality shares an association both historically and presently to medical institutions with other margin- alized sexual desires and behaviors. Yet, while activists and scholars have challenged the connections between medical discourses and same-sex desire (Conrad and Schneider, 1994; Kraft-Ebbing, 1886 [1959]; Rubin, 1984), diagnoses associated with asexuality (such as Sexual Aversion Disorder and Hyposexual Desire Disorder) are relatively unexplored. These similarities motivate collaboration in political strategy, as both asexual people and other sexual minorities who are in conversation with medical discourses might collaborate for a more complete transformation of these discourses. The lack of visibility and awareness of asexuality is a barrier to its inclusion in other sexuality-based political action groups.While a historical and contemporary relationship with discourses of medicine are shared, LGBTQ identities also have a historical relationship with legal institutions as gender presentation and same-sex behaviors have been prosecuted by legal institutions (D’Emilio, 1983; Rubin, 1984). Asexuality, on the other hand, has been largely unnoticed by legal insti- tutions, perhaps in part because of its lack of behavior and desire. In some ways, because asexuality is defined as a lack of behavior or desire, it has escaped attention, which is a clear departure from the experiences of other marginalized sexualities.
Asexual and LGBTQ groups also share similarities as both have created identity-based communities. As research documents, gay, lesbian, trans- gender and BDSM individuals use sexual identity communities to find support, relationships and to engage politically (D’Emilio, 1998; Rust, 1992). This is similar to how asexual individuals describe the functions of asexual communities. These communities not only serve similar functions, but both asexual and LGBTQ people are using internet technologies to form community (Jay, 2003; McKenna and Bargh, 1998; Turkle, 1995). While both utilize the networking possibilities of the internet, queer communities have additional visibility in physical spaces such as bars, bookstores and social service organizations that cater to LGBTQ ident- ities. Furthermore, there are cultural symbols that represent the desires, identities and behaviors of LGBTQ identities and subcultures (such as rainbows or pink triangles), whereas symbols of asexual identities and and subcultures are not yet generally recognizable. Thus, while both asexual and LGBTQ identities have identity-based communities, the forms and functions of these communities are distinct.
While the aforementioned aspects are more social-structural, asexuality shares a similar social-psychological process of coming to an identity as other marginalized sexual identities. As Paula Rust says, sexual identity is ‘a description of the location of the self in relation to other individuals, groups and institutions’ (Rust, 1996: 78). Given this understanding of sexual identity, bisexual, asexual, gay and pan-sexual individuals all draw on existing language, their current social situation and the social and cultural meanings associated with these identities to place themselves in relation to other individuals and institutions and to accurately describe their internal sense of self. Additionally, asexual individuals, as well as gay, bisexual or queer individuals, often share a sense of their sexuality as biological and innate, despite descriptions of coming to these identities that reveal profoundly social experiences.
In this article, I have described a few of the intersections between asexuality and other marginalized sexualities. This analysis is far from exhaustive, but it highlights the similarities between these sexualities and creates a need for further exploration of the overlapping social and political agendas of these marginalized sexualities. Not only are asexual identities interesting in their own right, but they contribute to a broader understanding of the construction of sexualities."
Marginalization in the Social Sphere
How Allosexuals Perceive and Interact With Asexuals
Prior to 2000, there was no research regarding perceptions of asexuality, and most assumed that asexual people did not face discrimination. A growing canon of work has emerged in the past decade showing that asexuals are routinely discriminated against and marginalized. The Development of The Attitude Towards Asexual Scale has laid the groundwork for a number of studies even within the past three years, and as time goes on this field will likely develop.Contact @asexualresearch on Twitter or [email protected] for articles that should be added, questions, or concerns!
Development and validation of the Attitudes Towards Asexuals (ATA) scale (Journal of Psychology And Sexuality)
“ Discomfort renting and hiring3
Discomfort renting to and hiring (MacInnis & Hodson, 2012) heterosexuals (α = .95), homosexuals (α = .96), bisexuals (α = .96) and asexuals (α = .98) was assessed using four items (e.g., ‘Indicate how comfortable you would be renting an apartment to people from each of these groups?’), rated on 11-point scales, with separate 4-item measures for each group. Scores were reverse-coded, with higher scores indicating greater discomfort rent- ing and hiring.”“ Interest in future contact (Husnu & Crisp, 2010) with heterosexuals (α = .92),
homosexuals (α = .94), bisexuals (α = .94) and asexuals (α = .91) were captured
using four items (e.g., ‘If given the chance, how interested are you in being friends
with someone from each of the following groups?’) rated on 8-point scales, with
separate 4-item measures for each group. Higher scores indicate greater future contact intentions.”
LGB within the T:
Sexual Orientation in the National Transgender Discrimination Survey and Implications for Public Policy
(This study examines sexual orientation and discrimination experienced by transgender people, an important step in analyzing the intersectionality of gender identity and sexual orientation.An important note about the data: Although only 264 asexual people responded, the researchers analyzed the data to make sure it was significant. The data with two asterisks are statistically significant, and those with one are statistically significant in the context of the complete study.)
Age of Participants (Interestingly, asexual respondents skewed older)
Familial Rejection
Public Accommodations And Incarceration
Housing
Racial and Ethnic Differences in Experiences of Discrimination in Accessing Social Services Among Transgender/Gender-Nonconforming People (Journal of Ethnic & Cultural Diversity in Social Work)
“The only difference on sexual orientation was that individuals who identified as asexual were more than twice as likely (OR = 2.37, 95% CI = [1.03, 5.46]) to have experienced discrimination at domestic violence shelters than heterosexual individuals.”
National LGBT Survey 2017 UK
The link above leads to the interactive data set. In the PDF library I have also included the analysis provided by researchers that the quotes arise from.
“Amongst cisgender respondents, gay and lesbian respondents were the most satisfied, compared to those with other sexual orientations, with an average rating of 6.88. Asexual and pansexual respondents were the least satisfied, with an average of 5.88 and 5.92 respectively (Figure 4.1).”“ Trans respondents had a lower life satisfaction, scoring it on average 5.40, than cisgender respondents, who scored it on average 6.67. Amongst trans respondents, trans men in particular were the least satisfied, scoring their life satisfaction on average 5.07 (Figure 4.2). Heterosexual trans respondents rated their life satisfaction the highest, scoring it on average 5.91, whilst asexual trans respondents rated it the lowest, scoring it on average 5.06 (Annex 4, Q152).”“Amongst cisgender respondents, gay and lesbian respondents were the most likely to score their comfort being LGBT in the UK as 4 or 5 out of 5 (63%), whilst asexual respondents were the least likely (49%) (Figure 4.4). Cisgender men were more likely to score their comfort as 4 or 5 out of 5 (63%) than cisgender women (54%) (Annex 4, Q11).”“ By sexual orientation, only 2% of gay and lesbian respondents had been open with none of their friends, whilst 12% of asexual respondents had been open with none of their friends (Figure 5.2). [greatest and least of the results]”“Openness with neighbours was generally low across sexual orientations, ranging from 39% of gay and lesbian respondents to 95% of asexual respondents having been open with none of their neighbours (Figure 5.6).”“ Broken down by sexual orientation, asexual respondents (89%), queer respondents (86%), and bisexual respondents (80%) were the most likely to avoid being open, compared to, for example, gay and lesbian respondents (66%) (Figure 5.11).““Fifty-eight per cent of asexual respondents said that they avoided being open about their sexual orientation at home, whereas only 14% of gay and lesbian respondents reported doing so. Some of this difference may reflect patterns of relationships and who lives with whom.”
On a scale of 1 to 5, how comfortable do you feel being an LGBT person in the UK? If you would prefer not to answer, please leave blank.
Overall, on a scale of 1 to 10, how satisfied are you with your life nowadays?
Do you ever avoid being open about your sexual orientation for fear of a negative reaction from others?
Where do you avoid being open about your sexual orientation for fear of a negative reaction from others?
In the past 12 months, did you experience any of the following from someone you lived with for any reason?
In the past 12 months, how many family members that you lived with, if any, were you open with about being LGBT?
In the past 12 months, how many people you lived with, if any, were you open with about being LGBT?
Think about the most serious incident in the past 12 months. Which of the following happened to you?
Who was the perpetrator(s) of this most serious incident?
Did you report this most serious incident?
Why did you not report this most serious incident to the police?
In the past 12 months, did you experience any of the following from someone you were not living with because you are LGBT or they thought you were LGBT? For example, from a friend, neighbour, family member you don't live, or a stranger. Please only include incidents that you haven't already told us about in this survey.
In the past 12 months, how many people in the following groups, if any, were you open with about being LGBT - Family members you were not living with?
In the past 12 months, how many people in the following groups, if any, were you open with about being LGBT - Friends you were not living with?
In the past 12 months, how many people in the following groups, if any, were you open with about being LGBT - Neighbours?
Think about the most serious incident in the past 12 months. Which of the following happened to you?
Who was the perpetrator(s) of this most serious incident?
Did you or anyone else report this most serious incident?
Why did you not report this most serious incident to the police?
Viewer Perceptions of and Attitudes Towards Asexuality in Response to Entertainment Media Representation (University of Twente)
"A Tukey post hoc test showed that the difference was between religious and non-religious participants on both the first (p = .001) and second (p < .001) measurement. On the second measurement, there was also a statistically significant difference between religious and ‘other’ participants (p = .045). The attitudes held by non- religious participants were therefore significantly more positive towards asexual individuals than the other groups in the respective measures.On the second question, ‘What is your opinion of the main character?’, 28.8% of respondents in the asexual condition, and 46.4% of participants in the unrelated condition, had a positive tone. There was a significant difference in tone between the conditions on the second open question [F(1,106) = 6.65, p = .011], with a mean score of 36.73 (SD = 36.78) with an average of 3.49% of the text reflecting positive emotions and 5.69% negative emotions in the asexual condition and 55.45 (SD = 38.52) with an average of 7.06% positive and 2.48% negative emotions in the unrelated condition. The difference between the asexual and unrelated conditions in positive emotions expressed was significant [F(1,106) = 4.33, p = .040], as was the difference between negative emotions [F(1,106 = 4.01, p = .048]. This shows that on the second open question, participants in the asexual condition had a less positive valence than the unrelated condition, and they also expressed overall less emotions. Of the emotions expressed, the asexual condition texts contained more negative than positive emotions, which was reversed in the unrelated condition.Although the greatest difference was expected to those that identified as “Conservative”, the fewer negative emotions expressed by “Liberals” compared to other groups was expected based on prior research. Aside from this, it was not expected that those who are “Non-political” have comparatively very low percentages of negative emotions in their texts, as previous studies have concluded that those who are more politically interested generally hold more positive attitudes to members of the LGBT community (Lee & Hicks, 2011; Norton & Herek, 2012; Whitley, 2001; Woodford et al., 2012). "
Judging an absence: Factors influencing attitudes towards asexuality (Trinity Western University Department of Psychology)
“Participants
The sample consisted of 1297 participants (48.6% women, 43.2% men, 6.4% nonbinary / other, 0.6% questioning) recruit- ed via sample-collecting and LGBTQ+ pages on social media sites. Gender was assessed through self-identification in an open-answer format. Some analyses were conducted with few- er cases due to missing data. The data were collected in Winter 2018 following IRB approval. Participants were informed that they were taking part in a study about perceptions of sexual minorities. All participants were required to be the age of ma- jority in their place of residence. Exclusion criteria included age below the age of majority, self-reported dishonesty, or a clear, consistent pattern of nonsensical responses. No compensa- tion was provided for participation in the study. Participants self-identified as non-LGBTQ+ (44.5%; n = 576), nonasexual LGBTQ+ (43.9%; n = 569), or asexual (11.0%; n = 143). Mean age was 25.9 (SD = 8.97; age range = 18–73). The sample was pri- marily North American (Canada, the United States, and Mexico; 72.0%; n = 935), with a majority speaking English as a first lan- guage (79.2%; n = 1028). 84.1% (n = 1091) of the sample report- ed at least some college or university or college education.
Measures
Participants completed baseline measures assessing demograph- ics, familiarity and attitudes towards asexual individuals, trait characteristics (openness, social dominance, right wing author- itarianism), behavioral intentions, and attitudes towards single people. This study uses a subset of measures taken from a larger study on attitudes and behaviors towards sexual minority groups.
Singlism
30 items were used to measure negative stereotyping of sin- gle persons (e.g., “It’s only natural for people to get married;” Pignotti & Abell, 2009). Higher scores indicate a more negative view of single persons (Cronbach’s α = 0.94 in the present sam- ple). This scale was included for the purpose of differentiating between antiasexual bias and bias against celibate or otherwise nonasexual single individuals.
Openness
Openness was measured using a 10-item subscale of the Big-Five Personality Inventory (e.g., “I see myself as someone who has an active imagination;” John, Donahue, & Kentle, 1991). Higher average scores indicated a more open personality; reliability in the present sample was Cronbach’s α = 0.72.
Social dominance orientation
The 16-item Social Dominance Orientation Scale was used to measure social dominance (Pratto, Sidanius, Stallworth, & Malle, 1994). A sample item is, “To get ahead in life, it is sometimes nec- essary to step on other groups.” Higher average scores represent stronger social dominance orientation. Reliability in the present sample was Cronbach’s α = 0.93.
Right wing authoritarianism
Zakrisson’s (2005) 15-item short form of the Right-Wing Authoritarianism scale was used to assess degree of authori- tarianism. A sample item is, “It would be best if newspapers were censored so that people would not be able to get hold of destructive and disgusting material.” Higher total scores repre- sent a stronger inclination towards right wing authoritarianism. Reliablity in the present sample was Cronbach’s α = 0.86.
Familiarity
Participants were asked to indicate whether they know anyone who is asexual. Those who indicated yes were then asked to rate from 1–7 the closeness of the relationships. We revised Hoffarth et al.’s (2016) definition of asexual to read: “people who have [little to] no sexual attraction to either sex (and never have).” The definition was revised to be in accordance with a more nu- anced understanding of asexuality that recognizes that some identities within asexuality may involve varying degrees of sex- ual attraction under particular conditions (Carrigan, 2011; Van Houdenhove et al., 2015a). Restricting asexuality to those who never experience sexual attraction under any condition could be a form of gatekeeping or an extension of asexual-exclusionist discourse (Donaldson, 2018; Hoins, 2017; Mosbergen, 2017).
Future contact and discrimination intentions
Following the lead of Hoffarth et al. (2016), interest in future contact (Husnu & Crisp, 2010) was modified in the present study to ask about the likelihood that an individual would have a con- versation, a friendship, or a dating relationship with an asexual person. Higher scores reflect a greater likelihood of future con- tact intentions with asexuals.
Discrimination intentions were assessed using a further 2 questions that asked about comfort with renting to and hiring asexuals. A sample item is, “How comfortable would you be with renting an apartment to someone who is asexual?”). Higher scores reflect a lower likelihood of discrimination intentions.
Attitudes towards asexual individuals
16 items were used to measure attitudes towards asexual individ- uals (Hoffarth et al., 2016; sample item: “People who identify as asexual probably just want to feel special or different.”). Higher average scores indicate a higher bias towards asexual individuals; reliability in the present sample was Cronbach’s α = 0.91.
RESULTS
Means and correlations for the key study variables are presented in Table 1. Nearly all respondents (91.52%; n = 1187) indicated at least moderate familiarity with the concept of asexuality. 46.03% (n = 597) know one or more asexual individuals. All study variables were associated with each other, which is unsurprising given the size of the study sample and the reliance on the litera- ture to select the study variables. However, most associations are either small or moderate, which minimizes concerns about col- linearity. Men were somewhat more than were persons of other genders to report negative attitudes (r = −0.31, p < .01). A small inverse association was found between openness and negative attitudes towards asexual individuals (r = −0.13, p < .01). Right wing authoritarianism was moderately associated with antiasex- ual bias, including negative attitudes (r = 0.46, p < .01), as was so- cial dominance orientation (r = 0.49, p < .01), as well as singlism (r = 0.53, p < .01).
We used multiple regression to test predictors of attitudes towards asexual individuals using a backward elimination pro- cedure (Table 2). A total of 9 independent variables were tested for inclusion in the model: age, gender, orientation, singlism, openness, social dominance orientation, right wing authoritar- ianism, knowing an asexual individual, and having a close rela- tionship with an asexual individual. Variables were kept in the model if p < 0.05. Results indicated that orientation (β = −0.15, p < .01), social dominance orientation (β = 0.33, p < .01), right wing authoritarianism (β = 0.02, p < .01), having a close rela- tionship with an asexual person (β = −0.03, p < .01), and sin- glism (β = 0.01, p < .01) explained 46.7% of the variance in atti- tudes towards asexual individuals (R2 = .47, F(5, 926) = 163.98, p < .01).
We also compared participants on attitudes towards asexual individuals based on three broad groups of self-reported orien- tation: non-LGBTQ+, nonasexual LGBTQ+, and asexual. While some participants indicated multiple overlapping identities, no participant was assigned to more than one group for the purpose of these analyses. Any indication of LGBTQ+ identity was sort- ed as LGBTQ+, unless the participant also reported an asexual identity (for example, participants who described themselves as asexual, demisexual, or aromantic). Heterosexual participants who did not indicate identification with either asexual or other LGBTQ+ identities were allocated to the non-LGBTQ+ group.
A one-way between subjects ANOVA comparing the effect of orientation (non-LGBTQ+, nonasexual LGBTQ+, and asexual) on attitudes found a statistically significant difference between orientations [F(2, 1063) = 48.87, p < .01]. Games-Howell post hoc comparisons showed that the mean scores for non-LGBTQ+ individuals (M = 2.13, SD = 1.31) were higher compared to non- asexual LGBTQ+ participants (M = 1.58, SD = 0.89) and asexual individuals (M = 1.36, SD = 0.35; M = 1.33). The differences be- tween the mean scores of nonasexual LGBTQ+ individuals and asexual individuals were not significant.”
Societal Challenge and Depression, Self-Esteem, and Self-Concept Clarity in Asexuals (University of Colorado Boulder)
“ About half of the asexuals (54%) chose three or below on the scale when asked how open they were with their families. Most stated that they hid their identity because their family was homophobic and would likely not react well to a nonstandard sexual orientation, or that past attempts to be open had received negative responses. Those who were open with their family often felt that they were misunderstood regardless of how open they were, and that their parents were displeased. One subject noted that when she ‘came out’ to her mother, she convinced her to keep it hidden from the rest of the family.
The majority (69.4%) of the asexuals who participated in the survey stated that they felt that their identity as an asexual had been challenged in the past. Those who felt they had had their identity challenged were most likely to have had it challenged by their friends, with family coming in second. Participants were least likely to have their identity challenged by an authority figure or their significant other, though approximately 14% of participants did have difficulty with their significant other’s views of their identity. “
UK National LGBT Survey 2020
"On average, respondents were less satisfied with their life nowadays than the general population, scoring it 6.5 out of 10, compared with 7.7 for the general UK population.9 Among cisgender respondents, gay/lesbian people had the highest scores (6.9) and pansexual or asexual people had the lowest scores (both 5.9). Trans people had low scores: trans men scored 5.1, trans women scored 5.5 and non-binary people scored 5.5.Average life satisfaction (out of 10)
Change between chart and table
UK Population 7.7
Gay/Lesbian 6.9
Bisexual 6.3
Pansexual 5.9
Asexual 5.9
Trans woman 5.5
Non-binary 5.5
Trans man 5.1UK Population
7.7
Gay/Lesbian
6.9
Bisexual
6.3
Pansexual
5.9
Asexual
5.9
Trans woman
5.5
Non-binary
5.5
Trans man
5.1Over half of the respondents (56%) felt comfortable being LGBT in the UK, rating their comfort as a 4 or 5 out of 5. Amongst cisgender respondents, gay and lesbian people were the most comfortable (63% comfortable) and asexual people were the least (49% comfortable). As with life satisfaction, trans people generally felt less comfortable. 37% of trans women, 34% of trans men and 38% of non-binary people felt comfortable being LGBT in the UK. Only 5% of all trans respondents aged under 25 said they felt very comfortable (scoring 5 out of 5), rising to 15% of those aged 55-64 and 31% of those aged 65+.
Safety
The existing evidence suggests that LGBT people are at greater risk than the general population of being victims of crime; Stonewall, for example, recently found in their YouGov survey that more than 25% of trans respondents who were in a relationship in the last year had been subject to domestic abuse.10 NIESR found that underreporting of hate crime is a particularly common issue. They also found that LGBT people can be unwilling to use relevant services for fear of homophobic, transphobic or biphobic responses from staff and service users or because they do not think the response will meet their needs. Data from the Crime Survey for England and Wales (CSEW) being published alongside this report for the first time reveal that gay, lesbian and bisexual people are more likely than heterosexual people to be victims of all CSEW crime.Openness about being LGBT
Over two thirds (68%) of all respondents with a minority sexual orientation said they had avoided holding hands in public with a same-sex partner for fear of a negative reaction from others. Similarly, 70% said they had avoided being open about their sexual orientation for fear of a negative reaction; this was higher for cisgender respondents who were asexual (89%), queer (86%), and bisexual (80%). The most common places where cisgender respondents had avoided being open about their sexual orientation were on public transport (65%) and in the workplace (56%). Some respondents described feeling safer moving to large cities with a significant LGBT population, like London, Brighton and Manchester."
Asexual and Non‐Asexual Respondents from a U.S. Population‐Based Study of Sexual Minorities (Archives of Sexual Behavior)
“Our hypothesis that asexuals would experience more stigma than non-asexuals was generally confirmed. Asexuals reported feeling more stigma than non-asexual men and women and more everyday discrimination than did non-asexual men. These results suggest that asexual identity is more stigmatized in society than LGB sexual minority identities. This supports prior research of MacInnis and Hodson (2012) who found that Canadian university students and online participants were more biased toward asexuals than toward LGB people. It also sup- ports the qualitative research of Gupta (2017) who interviewed 30 participants recruited from AVEN and other websites, and found that over half indicated that they had been stigmatized
or marginalized for being asexual. In Gupta’s study every par- ticipant mentioned at least one negative incident, such as get- ting medical or psychological explanations when they came out to family or friends, and feeling alienated from social events, classroom discussions about sex, conversations with friends, or media programs or advertising.“
Polish Asexualities: Catholic Religiosity and Asexual Online Activisms in Poland
“The report suggests that, much like other sexual minorities, asexuals are at a serious disadvantage in terms of mental health, social isolation, and social acceptance in Polish society (Świder and Winiewski 2017). For example, 22.9% of asexual people in the study indicated unfair treat- ment by the medical establishment, 21.9% mistreatment in their work- place, and 54.8% in their religious communities (Świder and Winiewski 2017, p. 48). Further, less than half of the asexual people in the study suggested that they would evaluate their life on positive terms, 68.2% have experienced social isolation, and 20.5% have frequent or very fre- quent suicidal thoughts (Świder and Winiewski 2017, pp. 54, 55, 57).“
Asexual Identity in a New Zealand National Sample: Demographics, Well-Being, and Health
(A study on people's perceptions of asexuals)
“In line with prior work on social avoidance, asexual men also had higher coldness, social avoidance, and non-assertive personality scores. Asexual women had higher scores on coldness, vindictiveness, social avoidance, non- assertiveness, and exploitable personality inventory indices. It was speculated that these differences might be partially due to the discrimination faced by asexual people, and living in a soci- ety that places a considerable emphasis on sex (see also Chasin, 2015; Scherrer, 2008).”
Societal Challenge and Depression, Self-Esteem and Self-Concept Clarity in Asexuals (University of Colorado Boulder)
"Asexuals were most open about their asexuality with their significant other and tended to keep it mostly hidden around their family, strangers, and authority figures. In the case of coworkers, many asexuals stated that it was not their business, though there were occasions where they felt pressured to state their sexuality. Most who hid their asexuality from authority figures did so from doctors and therapists for fear of their lack of sexual attraction being misconstrued as a symptom of an illness or mental disorder. Those who kept their asexuality hidden from the LGBT community stated that they did so because they had had unpleasant experiences with the community in regards to their asexuality in the past, while some stated that they were open with the LGBT community online but kept their asexuality hidden offline. Asexuals were asked how open they were about their sexuality on a scale of one to seven, with one being the most hidden and seven being the most open. About half of the asexuals (54%) chose three or below on the scale when asked how open they were with their families. Most stated that they hid their identity because their family was homophobic and would likely not react well to a nonstandard sexual orientation, or that past attempts to be open had received negative responses. Those who were open with their family often felt that they were misunderstood regardless of how open they were, and that their parents were displeased. One subject noted that when she ‘came out’ to her mother, she convinced her to keep it hidden from the rest of the family.
The majority (69.4%) of the asexuals who participated in the survey stated that they felt that their identity as an asexual had been challenged in the past. Those who felt they had had their identity challenged were most likely to have had it challenged by their friends, with family coming in second. Participants were least likely to have their identity challenged by an authority figure or their significant other, though approximately 14% of participants did have difficulty with their significant other’s views of their identity. The vast majority of challenges to asexuality that participants reported were phrases such as “you are a late bloomer” or “you have not met the right person.”The majority of the people who identified as asexual (69.4%) reported that they had their identity challenged in the past. It seems that the majority of asexuals, nearly 70%, have had their identity challenged or denied at some point and, judging by their comments, this has happened multiple times to many of them. The participants were the ones to decide whether they had been challenged or not, so it is possible that some people who may have had their identity challenged or denied by one definition did not by another, or vice versa. It is also possible that there are a number of people who have not had their identity denied because they keep their asexuality hidden from others for fear of rejection. Some who reported having their identity challenged may have not had it challenged directly; they may have seen something denying or discrediting asexuality on television or in a book. It may be worthwhile to see how this percentage compares to other sexualities and groups in the future. Asexuality as an orientation is a relatively new concept, and it is possible that things will change over time. LGB groups were hidden groups in the past, and LGB characters in the media started out as novel or stereotyped, but now LGB characters are relatively common, and tend to avoid stereotypical portrayals. Over the next decade or so we can probably expect to see asexuals and other non-standard sexual orientations, romantic orientations, and gender identities become more visible in the media, and in public discussions."
Asexuality: An Emergent Sexual Orientation (University of Saskatchewan)
"In response to the HHDRS items, participants reported experiencing a variety of
discriminatory behaviours, and hearing verbal insults on account of one’s asexual identity (15%), derogatory names being used to describe asexuals (13%), and anti-asexual remarks from family members (10%) emerged as the most frequently occurring events (see Table 1). These experiences, along with being treated unfairly by parents due to one’s asexual identity were pereceived as being stressful to varying degrees by 33%, 21%, 21%, and 23% of the sample, respectively. When examining the mean stress levels and ranges of stress evaluations for each experienced discriminatory episode (see Table 1), it is apparent that participants did not perceive the events to be overly stressful (possible range for these evaluations was 1-10, and the highest mean evaluation for any event obtained was 1.79, which participants perceived when verbally insulted due to their asexual identity). Moreover, participants’ total mean scale score (M = 23.14, SD = 9.90) on the HHDRS fell well below the scale midpoint of 84 and, thus, the sample experienced the types of discriminatory events included in the HHDRS relatively rarely.
Of interest, too, in the present study was obtaining an indication of the extent to which participants had disclosed their asexual identities to individuals of varying interpersonal closeness, as outlined on the OI. Percentages of participants who had disclosed their asexual orientation to each person/group of people were calculated, excluding those who responded with “not applicable” to any given item. Results indicate that most participants (85%) had disclosed their asexual orientation to at least one person, and a further 10% reported that they intend to disclose their asexual orientation in future. Participants’ responses were then divided into those who had disclosed their asexual identities and their identities were “definitely known” (i.e., responses on the OI of 5, 6, or 7 were given indicating that there was no uncertainty about participants’ disclosure) versus those who perceived to have disclosed their identity but the recipient of the information “probably knows” (i.e., responses on the OI of 1, 2, 3, or 4 were given indicating that a lack of certainty exists about the extent to which the person/group of people knows about a person’s identity). As seen in Table 2, of those participants who were certain that the individual/group in question definitely knows of their asexual identity, each had disclosed to his/her romantic partner, and over half of the applicable sample had disclosed totheir mental health care providers, old heterosexual, old non-heterosexual, and new non- heterosexual friends. Less than half of the applicable sample, however, had disclosed their identities to the remaining contacts listed on the OI.
Finally, the correlations between the HHDRS and the total OI, and the HHDRS and the OI subscales were calculated to determine the degree of association between the two measures. Scores on the HHDRS were significantly correlated with total OI scores, r(34) = .42, p = .01, scores on the religion subscale, r(35) = -.44, p = .01, and scores on the world subscale, r(34) = .50, p = .001. Scores on the HHDRS and the family OI subscale did not correlate significantly, r(35) = .30, p = .08. Overall, scores on the HHDRS and OI appear to be moderately associated.
DISCUSSION
To the authors’ knowledge, the present study is the first empirical investigation into
asexual individuals’ experiences of discrimination. In addition to measuring the types and sources of discrimination, a basic measure of the stress engendered by each experience from the participants’ perspectives was included. Further, the degree to which participants had disclosed their asexual orientation to various others also was investigated.
Responses to the OI indicate that a large majority of the sample had disclosed their asexual orientation to at least one person, and that almost the entire remainder of the sample was planning to do so in the future. This finding suggests that participants do not feel it necessary to completely hide their identity as asexual; however, the persons to whom they elect to disclose their identity was revealing. Specifically, only romantic partners, friends, and mental health care providers were those individuals to which over half of the sample had disclosed their identity as asexuals. Thus, although many participants had disclosed their asexual identity to at least one person, this aspect of their identity remains hidden from most of their proximal (e.g., family members) and distal (e.g., work peers and extended family) contacts. It is important to point out that the OI does not capture whether the disclosure of a participants’ asexual identity is deemed acceptable by others of varying interpersonal closeness. For example, although the OI measures whether one’s asexual orientation is openly discussed with one’s family members (e.g., brother/sisters), it does not measure whether the discourse is positive or negative in tone. Previous research has suggested that this discourse may, indeed, be highly negative and dismissive of asexuality and asexual relationships (Chasin, 2009; Scherrer, 2008, 2010). The inclusion of questions addressing the nature of the interactions with proximal and distal others would be useful.
With respect to the discrimination experienced by our sample, episodes of verbal harassment seem to be the most commonly cited. Specifically, insults, derogatory names, and anti-asexual remarks from family members due to one’s asexual identity were among the most frequent and stressful types of discrimination experienced. Based on these results, it seems that most participants had not experienced the types of blatant discrimination included in the HHDRS (e.g., physical violence or economic sanctions); however, the experiences reported suggest many perceive themselves to be living in environments in which their sexual identities are not accepted. The lack of perceived acceptance may fall under the rubric of subtle discriminatory behaviour (i.e., discrimination which is typified by acts that are derogative and hurtful, yet may or may not be ambiguous as to their prejudiced roots and intention to harm; Jewell, McCutcheon, Harriman, & Morrison, in press). For example, subtle discrimination may manifest itself in the form of gossip, use of anti-target language, and social distancing. Because the nature of subtle discrimination is not as well understood as its blatant counterpart (Jewell & Morrison, in press; Jewell et al., in press), the HHDRS is likely not as sensitive to the potential spectrum of subtle discriminatory behaviour experienced by asexual individuals. Some of the most frequently experienced events on the HHDRS, however, suggest that subtle discrimination may be an issue for the asexual community. For example, hearing anti-asexual remarks and being called derogatory names may be classified as subtle discrimination if the intent of the perpetrator was not to harm or ambiguous.
The family of origin seems to be a particular source of discrimination for asexual persons. Family members were conspicuously absent from the list of people to whom over half of the sample had disclosed their asexual identities. Indeed, participants reported disclosing their asexual identity less frequently to extended family members than to strangers. Again, the results of the OI do not indicate whether family members are accepting of participants’ asexual identities or not. However, the finding that family members were involved in two of the most frequent and stressful events on the HHDRS (i.e., unfair treatment by parents and anti-asexual remarks from family members) suggests that the familial environment can be negative for many asexual individuals.
The positive correlations between the HHDRS and the OI subscales suggest that participants who had disclosed their asexual orientation to others were also more likely to report experiencing the type of discrimination measured by the HHDRS. This result was anticipated because most of the HHDRS items refer specifically to discriminatory events that are precipitated by one’s asexual orientation. For example, to be rejected by a friend due to one’s asexual orientation, that friend would have to be aware that one is, in fact, asexual. One caveat to this conclusion was the negative correlation between the religion subscale and the HHDRS. Thus, participants who had disclosed their asexual orientation to members of their religious community reported fewer incidents of discrimination on the HHDRS. It may be that asexual individuals who are part of a religious community are more likely to be accepted by their acquaintances, or it may be that participants were more likely to disclose their asexual orientation to their religious community when they believed that it would accept their orientation. The present data, however, do not provide definitive conclusions regarding this relationship; thus, additional research designed to illuminate the nature of this association should be conducted."
“How do you Say ‘I’m Asexual’? It is even Difficult to Say”: The Construction of Asexual Masculinities in the Context of Sexual Imperative (From the Department of Philosophy, Sociology, Education & Applied Psychology, Università degli Studi di Padova, Padova, Italy)
“Overall, the results of our study are in line with earlier investigations about asexualities (DeLuzio Chasin, 2011; Gupta, 2015; Przybylo, 2011, 2012) and the link between nonsexuality and masculinity (Lopez Ruiz, 2015; Przybylo, 2014). The sexualization of interpersonal relationships appears to be a core dynamic in the cultural production of masculinity, as signaled by the precarious position occupied by asexual men in the domain of manhood. Specifically, the analysis of the interviews suggests that the delegitimation of asexual masculinities is performed in two ways: erasure and stigmatization.
Erasure relates to the scarce recognition of the disengagement from sexuality as a manifestation of a non- sexual identity. As previously emphasized by other authors (Gupta, 2017), our work points out that one of the major obstacles to the public visibility of asexuality is the difficult of finding definite and univocal behaviours to materialize one’s own asexual identification in the social field. Asexuality is largely, but not exclusively, narrated in terms of “lack” (see also DeLuzio Chasin, 2013; Przybylo, 2011) – of sexual desire, of sexual behaviours, of sexual attraction, of sexual pleasure – and the intelligibility of these manifestations of non-sexuality as an expression of asexuality is hindered by their reiterated misinterpretation as signs – or symptoms – of other sexual conditions (e.g. erectile dysfunction, shyness, latent homosexuality). In other words, asexuality is denied an independent ontological status in the field of masculinity as it is treated as a mere contingent epiphenomenon of other subordinated sexual masculinities.
The stigmatization refers instead to those situations in which asexuality, despite being regarded as an identification, is subjected in itself to emasculation, discrimination and other offensive behaviours. It is worthy of attention that the interviewees reported that their asexuality not only has been treated as more unacceptable than homosexuality, but also it has been denigrated even by men who identify in non- normative sexual orientations. This result seems to implicate that asexualities are placed in a perhaps moreprecarious and subordinated position in the field of manhood as compared to other non-normative sexual identities. This is in agreement with MacInnis and Hodson’s (2012) results about the higher rates of dehumanization towards asexual people and asexual men in particular.
Both in erasure and in stigmatization asexuality is sanctioned and delegitimated. Nonetheless, we believe that the process of erasure and misrecognition constitutes a specific form of violence (see Fine, Torre, Frost & Cabana, 2018) that goes beyond what has been identified as subordination in the scholarship about hegemonic masculinity. Indeed, in this case the link between masculinity and sexual desire is so intense that asexuality cannot occupy any position in manhood, not even a subordinate one: the existence of asexual masculinities is ignored or actively rejected. As a consequence, the behaviours and desires of asexual-identified men can enter in the field of intelligibility of masculinity only after being subjected to colonization by the sexual imperative, as they are redefined as yet another defective expression of the ubiquitous sexuality.
The relationship between asexual identities and the subordination of non-sexualities in the field of masculinity is far from linear. Even though asexual men are, as we discussed earlier, extensively targeted by emasculating stereotypes, we are persuaded that the asexual identification opens up a certain space for renegotiating the location of one’s own non-sexuality within or outside the available cultural definitions of masculinity. As maintained by Gupta (2017; see also Scherrer, 2008), the very existence of a term to materialize one’s own disengagement from sexuality as an identity provides a symbolic tool to create – in self-narratives, in social interactions and in public speech – a discursive space outside sexuality. Indeed, it being understood that asexuality is still far from being socially accepted, the shift from the almost complete inexpressibility of non-sexual subjectivities to the possibility to articulate the existence of asexuality envisages at least tensions and fractures in the sexual imperative and in the male sexual drive discourse. This process echoes other researchers’ conclusions about the disruption of heteronormativity produced by the emergence and visibility of sexual and gender non-normative identities (Bruce, 2013; Gamson, 1995; Malici, 2014, Primo, Zamperini, Testoni, 2019; Skeggs, 1999), and it is particularly cogent given the difficulties in making manifest one’s own non-sexuality. Claiming an asexual identity opens up a discursiveniche in the language of subjectivity from which it is possible to reject the dominant hypersexual connotation of masculinity. Nonetheless, the relationship between the stabilization of asexual identities and the social recognition of non-sexuality in general is controversial. Indeed, the constitution of a symbolic domain of asexuality is achieved also through the demarcation of a distinction between asexuality and other non-sexualities, as already pointed out by Flore (2013). Notably, in the case of masculinity the asexual identification can also enact a partial displacement of the emasculating stigma towards other non-sexual conditions, especially those who are commonly labelled as “sexual dysfunctions”.
To conclude, the findings of this study appear to provide further support to the growing belief that normative conceptions about the appropriate level of engagement with sexuality are at the core of the cultural organization of meaning associated with masculinity. In particular, we concur with previous works in this area in suggesting that asexual men inhabit an extremely precarious position in gender dynamics. The social rejection of non-sexual masculinities is so intense and widespread that they are not only subjected to subordination, but also to more radical forms of erasure and symbolic colonization. In addition, we believe that our inquiry provides important insights about the complex and multifaceted roles that the asexual identification plays in the constitution of non-sexual male subjectivities. As we emphasized, this relates not only to the renegotiation of the hegemonic position of heterosexual masculinities, but rather to a broader web of symbolic and material relationships that involves also non- normative sexualities and other non-sexual conditions. For this very reason, we suggest that a compelling topic for future research in the CSMM scholarships is the investigation of the heterogeneous interrelations among different subordinate locations in the field of manhood.”
Asexual People’s Experience with Microaggressions (City University of New York)
(This study is a 45-page document detailing the types, sources, and effects of microaggressions. For space restrictions, I have only included the conclusion.To read the complete study, check out the library.)“This study was done to discover if asexual people experience microaggressions, and if so, how the microaggressions manifested, who they came from, and what mental health effects they may have. Information from this study was also collected to inform further research, as well as increase competency for mental health care providers that have asexual clients. This study supports the proposition that asexual people do experience subtle discrimination known as microaggressions. The themes found were similar to the themes found in other research on LGBTQ identities (Nadal, 2011). The microaggressions came from the expected sources similar to other microaggression studies, such as family, friends, and the media. They did report some more overt forms of discrimination in the form of attempted sexual assault and nonconsensual touching that appeared to intersect with their gender identity; the participants all identified as women and women report a 1 in 5 rate of rape in the United States (NSVRC, 2015).
Discrimination has long been associated with negative mental health outcomes and distress, and microaggressions are starting to be associated with negative mental health outcomes as well (Nadal, 2011). It is important to know that asexual people are facing this form of discrimination and how it affects them so it can be combated and access to support and needed mental health care can be provided. Microaggressions also can come from healthcare providers and even mental health providers, as indicated in this study and others (Shelton & Delgado-Romero, 2011). Providers should be able to recognize the common microaggressions against asexual people so that they can avoid perpetuating microaggressions in the future and they can provide more competent and compassionate care. Microaggressions and discrimination have been previously shown to have negative effects on the mental health of LGB individuals, and the asexual participants in this study reported that microaggressions caused them increased anxiety, relationship stress, discomfort, and depression. Considering LGB people also report higher levels of mood disorders and personality disorders compared to heterosexual people, it is important to know what may be contributing to this, as they may be a population at a greater risk of negative mental health outcomes and in need of greater care (Yule, Brotto, & Gorzalka, 2013). They also may be seeking therapy more frequently because of their mental health and it is important to be culturally competent and aware of what asexual people face as a population. If health providers become aware of the experiences of asexual people, these individuals would be spared the need to explain their sexual orientation and freed from experiencing microaggressions in a health care setting where they need treatment.”
Intergroup bias toward “Group X”: Evidence of prejudice, dehumanization, avoidance, and discrimination against asexuals (Journal of Group Processes & Intergroup Relations)
Summary (written in Psychology Today article): In a recent investigation (MacInnis & Hodson, in press) we uncovered strikingly strong bias against asexuals in both university and community samples. Relative to heterosexuals, and even relative to homosexuals and bisexuals, heterosexuals: (a) expressed more negative attitudes toward asexuals (i.e., prejudice); (b) desired less contact with asexuals; and (c) were less willing to rent an apartment to (or hire) an asexual applicant (i.e., discrimination). Moreover, of all the sexual minority groups studied, asexuals were the most dehumanized (i.e., represented as “less human”). Intriguingly, heterosexuals dehumanized asexuals in two ways. Given their lack of sexual interest, widely considered a universal interest, it might not surprise you to learn that asexuals were characterized as “machine-like” (i.e., mechanistically dehumanized). But, oddly enough, asexuals were also seen as “animal-like” (i.e., animalistically dehumanized). Yes, asexuals were seen as relatively cold and emotionless and unrestrained, impulsive, and less sophisticated.-
Complete Findings: As predicted, attitudes toward heterosexuals (ingroup) were the most positive (see Table 1). Attitudes toward homosexuals, bisexuals, and asexuals were more negative than attitudes toward heterosexuals, revealing a sexual minority bias. Within sexual minorities, homosexuals were evaluated most positively , followed by bisexuals,
with asexuals being evaluated most negatively of all groups. Thus, not only are more negative atti- tudes leveled toward sexual minorities (vs. hetero- sexuals), but antiasexual prejudice is the most pronounced of all.Less favorable attitudes toward each sexual minority group were associated with increases in
RWA, SDO, ingroup (i.e., heterosexual) identifi- cation, or religious fundamentalism, as expected (see Table 2). Interestingly, relations between these prejudice correlates and attitudes toward asexuals are similar to relations between these variables and well-established sexual minority attitudes (i.e., attitudes toward homosexuals, bisexuals), despite the latter engaging in same- sex behavior whereas asexuals engage in no (or little) sexual activity. Prejudice-prone individuals, it seems, are biased against sexual minorities due to their deviant status rather than sexual actions perse.Attitudes toward sexual minorities (homosexuals, bisexuals, asexuals) were significantly and posi- tively intercorrelated, suggesting generalized sex- ual minority attitudes (see Table 2). That is, those liking (or disliking) homosexuals or bisexuals like- wise like (or dislike) asexuals. Furthermore, a confirmatory factor analysis supported a single factor of sexual minority prejudice: loadings .94 bisexual, .85 homosexual, .73 asexual.Trait-based dehumanization Uniquely human traits were perceived to apply most to heterosexu- als and were attributed less to homosexuals and bisexuals than heterosexuals (see Table 1). Asexu- als were attributed significantly lower uniquely human traits than any other sexual orientation group. Human nature traits were attributed signifi- cantly more to homosexuals than heterosexuals, bisexuals, and asexuals. Human nature traits were attributed significantly more to bisexuals than heterosexuals and asexuals, and heterosexuals were attributed significantly more human nature traits than asexuals. Thus, of the four sexual ori- entation groups, asexuals were perceived to be least “human” in terms of both uniquely human and human nature traits/characteristics.Emotion-based dehumanization A similar pat- tern emerged regarding perceived emotions expe- rienced by each group. Uniquely human emotions were perceived to be experienced most by homo- sexuals, followed by heterosexuals, and bisexuals; uniquely human emotions were perceived to be significantly least experienced by asexuals relative to all other targets. Human nature emotions were perceived to be most experienced by heterosexu- als and homosexuals, less by bisexuals (relative to heterosexuals and homosexuals), and experi- enced the least by asexuals relative to heterosexu- als, homosexuals, and bisexuals. As with trait-based dehumanization, asexuals were denied uniquely human and human nature emotions (see Table 1).Overall, participants indicated greater preference for future contact with heterosexuals relative to sexual minorities. Within sexual minority groups, contact with homosexuals was preferred over con- tact with bisexuals or asexuals (see Table 1). Again, thisdemonstratesevidenceofantisexualminority bias, and contact least desired with bisexuals and asexuals(equivalently).Ofparticularinteresttothe present investigation, contact with asexuals was desiredsignificantlylessthancontactwithhomo- sexuals, a frequently studied prejudice target group.
Participants were most willing to rent to hetero- sexuals relative to sexual minorities. Following heterosexuals, participants were most willing to rent to homosexuals or asexuals, and least to bisexuals. The same pattern was observed with regard to hiring decisions (see Table 1). Overall, participants intended to discriminate against sex- ual minorities (including asexuals), with most bias directed toward bisexuals.Importantly, attitudes toward asexuals do not simply reflect negative biases toward single peo- ple. In fact, attitudes toward asexuals were not significantly related to singlism (see Table 2). Moreover, relations between RWA, SDO, ingroup identification, or religious fundamentalism and asexual attitudes remain relatively unchanged after statistically controlling for singlism (partial correlations equal −.41, −.31, −.29, and −.25, ps < .001, respectively).Empirically, very little is known about asexuality relative to other sexual orientations, and no research has addressed whether asexuals are tar- gets of bias at the group level. Addressing this lat- ter question for the first time, our analysis suggests that antiasexual prejudice is indeed a sexual minor- ity prejudice, correlating positively with attitudes toward homosexuals and bisexuals. Relative to the heterosexual ingroup, we find compelling evidence of antisexual minority prejudice, with this newly identified bias being particularly extreme. Strikingly, on many key measures (particularly intergroup evaluations, dehumanization, and for the most part, contact intentions), we find significantly more bias against asexuals than other sexual minorities, and discrimination intentions matching that against homosexuals. Overall, we find clear evi- dence of a previously unidentified and strong sex- ual minority prejudice: antiasexual bias.
In keeping with this bias being intergroup in nature, those higher (vs. lower) in RWA or SDO expressed particularly strong dislike of asexuals, as they typically do for deviant and low-status groups. In keeping with social identity theory, stronger heterosexual identification was also associated with greater asexual prejudice. This relation between heterosexual identification and favorable evaluations of asexual people became smaller when statistically controlling for RWA and SDO, but remained significant (rp = −.19, p = .022). Overall, negativity toward asexuals is marked by an ideological flavor that is clearly intergroup in nature, not a simple indifference toward a nonnormative other. Importantly, although those higher in SDO or RWA expressed greater singlism, their dislike of asexuals was not explained by singlism. Antiasexual bias is a type of sexual minority prejudice distinct from related constructs and rooted in ideological opposition to deviant sexuality (not merely those adopting independent or single lifestyles). That is, antia- sexual bias is not merely singlism.
Those higher (vs. lower) in religious funda- mentalism also demonstrated less favorable atti- tudes toward asexual people, despite asexuals being disinterested in sexual relations, a relation that remains after statistically controlling for SDO (rp = −.19, p = .019). Upon statistically control- ling for RWA however (rp = .05, p = .548), or both RWA and SDO (rp = .03, p = .698), this relation- ship reduces to nonsignificance. This latter find- ing is unsurprising, given that few variables predict prejudice above and beyond RWA and SDO (see Altemeyer, 1998). Further, strong correlations typically exist between RWA and religious funda- mentalism (r = .67 in the current study), leading Altemeyer and Hunsberger (2004) to consider religious fundamentalism a “religious manifesta- tion” of RWA. Thus, while evaluations of asexu- als are more negative among prejudice-prone individuals, asexual prejudice does not have a unique religious component, but rather reflects concerns with status quo and group dominance.
Our dehumanization results are particularly compelling. Asexuals (relative to heterosexuals) were dehumanized with regard to both dimen- sions (represented as animalistic, and particularly as machine-like), regardless of whether these assess- ments were based on traits (i.e., characteristics) or emotions (i.e., sensation capability). Generally speaking, asexual dehumanization was greater than that characterizing other sexual minorities, showcasing this bias as serious and extreme. Sexuality appears to be perceived as a key compo- nent of humanness. The dehumanization meas- ures employed did not explicitly reference sexuality, yet asexuals were strongly biased against on these measures. Thus, characteristics/emo- tions representing humanness are clearly inter- twined with sexuality and/or sexual desire.
The researchers then replicated the study with a new population.
Replicating Study 1, a sexual minority bias was demonstrated whereby attitudes toward heterosex- uals were the most positive, followed by attitudes toward homosexuals, bisexuals, and asexuals. Within sexual minorities, homosexuals and bisexu- als were evaluated equivalently, with asexuals evalu- ated more negatively than both homosexuals and bisexuals (see Table 3). Again, the pattern of antia- sexual prejudice, relative to the heterosexual ingroup and even relative to other sexual minorities was uncovered. Importantly, this general pattern of differential evaluation of sexual orientation groups matches that of Study 1, even though atti- tudes toward each group are more positive in the online (vs. student) sample (ps < .003).As in Study 1, less favorable attitudes toward sex- ual minority groups were associated with increases in RWA, SDO, heterosexual identification, or reli- gious fundamentalism. In one exception, attitudes toward asexuals were not significantly correlated with religious fundamentalism (see Table 4). Overall, associations between attitudes and RWA, SDO, and heterosexual identification corroborate our findings from Study 1: prejudice-prone indi- viduals are more biased toward asexuals, as they are toward other sexual minorities (note that, unlike Study 1, the relation between heterosexual identification and bias toward asexuals reduces to nonsignificance when statistically controlling for RWA and SDO, consistent with the notion that bias against asexuals is about conventionality, tra- ditionalism, and group dominance).As in Study 1, attitudes toward sexual minorities were positively intercorrelated (see Table 4) with a confirmatory factor analysis supporting a single factor of sexual minority prejudice: loadings .97
6 bisexual, .89 homosexual, .76 asexual .Uniquely human
traits were perceived to apply most to heterosexuals and homosexuals, and attributed less to bisexuals and asexuals than heterosexuals (see Table 3). Human nature traits were perceived to apply equiva- lently to heterosexuals, homosexuals, and bisexuals, with asexuals attributed significantly lower human nature traits than each of the other groups. Thus, evidence of antiasexual bias was again evident.Both uniquely human and human nature emotions were per- ceived to be experienced equivalently by hetero- sexuals, homosexuals, and bisexuals, and experienced significantly less by asexuals relative to each of the other groups. Again, asexuals were relatively denied uniquely human and human nature emotions (see Table 3).Confirming Study 1, heterosexuals indicated prefer- ence for future contact with heterosexuals relative to
sexual minorities. Desired future contact with homosexuals and bisexuals were equivalent, and contact with asexuals was even less desired than contact with homosexuals (see Table 3).A sexual minority bias was evident, whereby par- ticipants were most willing to rent to and/or hire heterosexuals relative to homosexuals, bisexuals, or asexuals (see Table 3).In Study 2, less favorable attitudes toward asexu- als were related to greater singlism (r = −.22), but not so much as to indicate strong conceptual overlap (see Table 4). Furthermore, relations between RWA, SDO, or ingroup identification and favorable attitudes toward asexual people remained significant after statistically controlling for singlism (partial correlations equal −.30, −.26, −.22, and ps < .03, respectively). These findings further corroborate the proposition that biases against asexuals concern their sexual deviancy rather than simple biases against those who are relatively independent and not in committed sex- ual relationships.As noted previously, bias against asexuals might reflect a bias against a relatively unfamil- iar sexual minority, rather than asexuality per se. This potential explanation, however, is not supported. Heterosexuals were not surprisingly the most familiar sexual orientation group (M = 8.90). Homosexuals (M = 8.51) were less familiar than heterosexuals, followed by bisex- uals (M = 7.92) (ps < .001). Asexuals (M = 5.80) were less familiar than heterosexuals, homosexuals, and bisexuals (ps < .001). As expected, sapiosexuals (M = 2.67) were deemed significantly less familiar than heterosexuals, homosexuals, bisexuals, and most critically, asexuals (ps < .001).
Although asexuals were not the least familiar sexual minority target, they were nevertheless the most negatively evaluated. That is, attitudes toward asexuals were significantly more nega- tive than attitudes toward sapiosexuals (M = 6.81), t(100) = 2.24, p = .027. If lack of famili- arity were solely responsible for the pattern of group evaluations obtained (see Tables 1 and 3), sapiosexuals would be the most negatively eval- uatedgroup.Infurtherevidencethatfamiliarity per se does not explain dislike of asexuals, rela- tions between RWA, SDO, or ingroup identifi- cation with asexual evaluations were relatively unchanged after statistically controlling for familiarity with asexuals (partial correlations equal −.36, −.31, −.24, and ps < .02, respec- tively). Prejudice-prone persons, therefore, were not more prejudiced toward asexuals as a result of mere unfamiliarity.Employing an online community sample, the results of Study 2 largely confirm those from the university sample examined in Study 1. Asexuals were evaluated negatively relative to both hetero- sexuals and other sexual minorities, with order effects not explaining this pattern given the rand- omized order of evaluations. Notably, asexuals were evaluated more negatively than a very unfa- miliar sexual minority comparison group, sapio- sexuals. The group lacking sexual desire, rather than the least familiar group, was the target of the most negative attitudes. Again, we provide evi- dence that antiasexual bias is a form of sexual minority prejudice, that those prone to prejudice are more prone to antiasexual bias, and that asex- uals are targets of dehumanization, avoidance, and discrimination intentions. Further, we dem- onstrate that bias toward asexuals is either equiva- lent to, or even more extreme, than bias toward homosexuals and bisexuals.
Although these results largely corroborate Study 1 some interesting differences emerged. First, mean evaluations of each group were noticeably more positive in Study 2. Interestingly, university students were more negative toward homosexuals, bisexuals, and asexuals than the population in general. This might come as a sur- prise given university students’ reported tendency toward liberalism and lower prejudices toward most other social targets (Henry, 2008). This finding suggests that university-aged students strongly value heteronormative sex, viewing sex- ual minorities, especially those preferring no sex at all, as deficient. Second, although asexuals were dehumanized on both dimensions (uniquely human and human nature) by the overall sample, sex differences emerged, whereby men repre- sented asexuals as animalistic more consistently than did women (see Endnote 5). There was a strong overall tendency however, as in Study 1, for asexuals to be viewed by both men and women as more machine-like than heterosexuals, homosexuals, or bisexuals. Overall, asexuals are clear targets of bias by heterosexuals.
Discussion of Findings In Both Studies
We have established consistently that asexuals are evalu- ated negatively (not due to a simple lack of famili- arity). Asexuals’ status as a highly atypical and “deficient” (Herek, 2010) sexual minority group seems to be a more likely source of this prejudice. We have established various forms of antiasexual bias (including dehumanization) relative to heter- osexuals and, in some cases, other sexual minority groups. Taken together, Studies 1 and 2 confirm the existence of antiasexual bias, in university and community samples, respectively.
Our findings are in keeping with Herek’s (2010) “differences as deficits” model of sexual orientation, where sexual minorities deviating from the norm are considered substandard and deserving of negativity by the majority. This model is gradually becoming less applicable to homosexuals and bisexuals with changes in soci- etal norms (Herek, 2010), consistent with our findings that homosexuals (and in some cases bisexuals) were viewed as equally or more human than the heterosexual ingroup . However, we
posit that asexuals fit well within the “differences as deficits” framework. Asexuals are the sexual minority that is most clearly considered “defi- cient” by heterosexuals. In keeping with this interpretation, themes relevant to maintaining the status quo and group dominance (RWA and SDO, respectively) proved consistently important in predicting antiasexual attitudes, whereas con- cerns with positive ingroup identity and religious fundamentalism were less uniquely important.
Although antiasexual bias is a clear compo- nent of sexual minority prejudice, it is also unique in that it was repeatedly stronger than bias toward other sexual minorities. Most disturbingly, asexu- als are viewed as less human, especially lacking in
terms of human nature. This confirms that sex- ual desire is considered a key component of human nature, and those lacking it are viewed as relatively deficient, less human, and disliked. It appears that asexuals do not “fit” the typical defi- nition of human and as such are viewed as less human or even nonhuman, rendering them an extreme sexual orientation outgroup and very strong targets of bias. Future research can address the mechanisms underlying this tendency.
“And Now I’m Just Different, but There’s Nothing Actually Wrong With Me”: Asexual Marginalization and Resistance (Study Published in the Journal of Homosexuality)
"A number of scholars studying asexuality have argued that although Western society is certainly “sex negative” in some ways, Western society also systematically privileges sexual identifications, desires, and activities while marginalizing different forms of non- sexuality, to the detriment of asexually identified individuals (for example, Chasin, 2013; Emens, 2014; Gupta, 2015a). According to some scholars, asexual commu- nity formation poses a challenge to this society-wide system of “compulsory sexuality” or “sex-normativity,” calling into question deeply held assumptions about sexuality and relationality (Chasin, 2013).A number of studies have explored one or more of the negative impacts of contemporary sexual norms on the lives of asexually identified individuals. According to this scholarship, asexually identified individuals can face pathologization (Foster & Scherrer, 2014; Robbins, Low, & Query, 2015), difficulties in relationships and social situations (Carrigan, 2011), and disbelief or denial of their asexual self-identification (MacNeela & Murphy, 2014).In response to a direct question about whether they had ever felt stigmatized or marginalized as a result of their asexual identity, more than one half of the interviewees answered “yes,” more than one quarter answered “maybe” or “in some ways yes, in some ways no,” and around 20% answered “no.” In addition, all the interviewees described at least one negative experience attributable to compulsory sexuality. Here I offer a typology of these negative impacts of compulsory sexuality: pathologization, isolation, unwanted sex and relationship conflict, and the denial of epistemic authority. It is important to emphasize that what follows should not be taken as direct evidence of marginalization, stigma, or discrimination but as the interviewees’ interpretations of and narratives about particular life experiences.Isolation and invisibility
When asked about experiences of stigma or marginalization or if they saw any
negative aspects to identifying as asexual, at least two thirds of interviewees
reported occasionally feeling isolated or alienated from others or from society as
a result of the stigmatization or invisibility of nonsexuality. For example, Hannah talked about avoiding restaurants, bars, and clubs to avoid feeling isolated: “I think that a lot of social activities are like that, a lot of people think the goal is to hook up...So I sort of don’t want to participate in these sorts of things.” Anne, a current undergraduate majoring in psychology, described feeling isolated during a classroom discussion about sex: “It’s sort of a lonely feeling...everyone was like laughing and so forth, and I was kind of like ‘Ha-ha-ha, I don’t really get it,’ you know?” Sharon, age 49, described being bullied as a child, which she attributed to her weight and social awkwardness and to her lack of interest in dating or sex. She said, “I know my general social awkwardness, especially then, was a big part of what made me a target for them, but I also think that the asexuality played a significant part as well. I didn’t react to those boys the way they wanted me to. I had no sexual interest in them, and didn’t know how to fake it.”
At least 12 interviewees described feeling left out when their friends or peers talked about sex. For example, Lilly, 19, stated, “There would be a sleepover and people would be like, ‘Let’s play truth or dare.’ And almost all the questions are like, ‘Oh, who do you like? Have you ever kissed a guy? Who do you have a crush on?’ And I’d just be sitting there, like, ‘I don’t have a crush on anyone.’ ... And usually they’re like, ‘Oh, you’re boring.’”
At least eight interviewees described feeling isolated as a result of what they perceived as the overwhelming sexualization of the media and advertising. Mark, 25, said, “And now there’s sex everywhere...Also, sex sells on television, commercials, television shows...It’s just—I feel like it’s everywhere.” At least seven interviewees reported feeling isolated because asexuality is not represented in the media. Lilly said, “And so definitely the main thing that we face is erasure...the number of [asexual] characters in books and movies and TV who openly identify as asexual is two...it’s hard to figure stuff out just because there’s no examples.”Denial of epistemic authority
Lastly, in response to a question about how others had responded to their (a) sexuality, almost two thirds of interviewees reported at least one experience where they had been denied epistemic authority in regard to their own
sexuality. In other words, according to these interviewees, they had been met with the reaction that they could not know that they were asexual—they were told that they could be late bloomers, they had not met the right person yet, or they were repressing their sexual desires. About this Hannah said, “They insist that you essentially are not mentally competent to make your own decisions about yourself, which is really insulting to imply. You’ve met them for five minutes and they automatically know that you can’t make decisions by your- self. Like that’s really rude.” This was a response that interviewees reported encountering even in some LGBT communities. Eleanor, 50, said, “Nobody will just say, ‘Cool, you’re asexual.’ ... Even among gays and lesbians—that’s the one that always freaks me out—that gay and lesbian people can’t under- stand since they have a unique sexuality. But I guess they feel like everyone should have a sex, want to have sex, be attracted sexually to people.” On the other hand, it is important to note that at least 17 interviewees also described an instance in which they received a supportive response upon coming out.
A mystery wrapped in an enigma – asexuality: a virtual discussion (Interview with prominent researchers in asexuality)
"How is the negativity directed toward asexual individuals similar to/different from the negativity directed at other sexual minorities (e.g., gay men, lesbian women, etc.)?
I imagine that the similarities in the negativity experienced would revolve around the ‘magic cure.’ How many times has a lesbian woman been told ‘all you need is a good fuck by a real man?’ As if a lesbian woman is only interested in women because she hasn’t ‘met the right man.’ I have personally been told that if I just slept with a woman I would ‘absolutely fuckin’ love it’ and I would be ‘normal.’ I would imagine the same would be true for asexual individuals, being told that all they need is sex with someone (of the opposite sex of course) to ‘cure’ them and make them ‘normal.’
– BishopWe need to remember that many asexual individuals also identify as gay, lesbian, bisexual, transgender, and/or queer, and thus may face the same types of negativity directed at other LGBTQ individuals. My general impression from the U.S. context is that the negativity directed at asexual individuals is similar in some ways to the negativity directed at other sexual (and gender) minorities: asexual individuals, like other sexual minorities, may be perceived as mentally or physically ill, asexual individuals may feel alienated in social settings organized to facilitate heterosexual coupling, and asexual individuals may be denied legal and/or social recognition of their most important relationships. On the other hand, to a perhaps greater extent than other sexual minorities, asexual individuals are often denied ‘epistemic authority’ in regards to their own (a)sexuality. In other words, asexual individuals may be met with the reaction that they can’t really know that they are asexual – maybe they haven’t met the right person yet, maybe they are ‘late bloomers,’ maybe they are unconsciously repressing their sexual desires, maybe there is a physical cause of their asexuality that simply hasn’t been found yet. It is also my impression that asexual individuals in the U.S. (who do not also identify as LGBTQ) do not seem to be widely subjected to some of the more virulent hostility directed at other sexual and gender minorities, such physical battering and employment discrimination.
– GuptaWhat directions do you expect asexuality research to take over the next decade?
I hope that at the very least future research will not focus on how to ‘fix’ asexual individuals and will instead focus on them as people and the struggles they face. I realize this is unlikely to happen as there will be labs out there funded by religious groups or other ‘crusaders’ who want to ‘help’ asexual individuals. But still, a guy can dream.
– Bishop"
Freedom and foreclosure: Intimate consequences for asexual identities (Journal of Family Relationships And Societies)
“These participants thought of themselves as being inherently different; as Lisa poignantly says here,“not even a proper human being”.This shows the two ways in which identity can occur via dissociation from others (Skeggs, 2005). First, one’s self-identity can shape what we think we can or cannot do and therefore the strategies we adopt. In this case, the lack of experience of sexual intimacy is foundational to Deena’s account – which she feels means that she cannot fully participate in her friendships. Consequently, Deena practiced faking with her female friends – she internalised the cultural script and, much like Immy, developed a way of ‘passing’ to hide what she believed was the discreditable stigma of her lack of sexual experience. She used this ‘cover story’ as a strategy of information control for the purposes of dramaturgical self-presentation (Goffman, 1959, 1963). Second, interactions and relations affect self-identity: being unable to relate to others about something that is so important to her made Lisa feel excluded and alienated.This inevitably affected her sense of self and reinforced the feelings of difference; of ‘not being a proper human being’.Therefore, here we see the ways in which the cultural ‘sexual assumption’(Carrigan,2012) can lead to forms of exclusion for those who do not fit within it.“
Mental Health Disparities by Identity Among Gender and Sexual Minorities (University of Minnesota)
"In addition, victims of LGBTQIA2S+ hate crimes are more likely to experience indifference and abuse from law enforcement when attempting to report the crime, another example of structural stigma which could compound the stress of being victimized in the first place (Hein & Scharer, 2012).
Asexual, bisexual, and trans people experience more marginalization in society in general, and although this marginalization extends to psychological research, the research that has been done shows that mental health disparities are more severe for these particular groups.
When comparing the different types of negative attitudes and bias of heterosexuals toward different sexual minority identities, it was found that regardless of whether bias was based on “right wing authoritarianism,” (bias based on ideology) or “social dominance orientation,” (bias based on cultural norms) heterosexuals had most negative attitudes and bias toward asexuals, followed by bisexuals, with homosexuals as the sexual minority receiving the least bias and negativity (MacInnis & Hodson, 2012). This demonstrates that there is more individual bias toward the more marginalized identities in order of marginalization, so bisexuals experience more negativity and bias directed toward them than gay or lesbian people, and asexuals experience even more. It is possible that this bias is directed toward identities perceived as more “deviant”: asexuals may be more deviant because they do not conform to the social expectation that everyone is interested in sex (MacInnis & Hodson, 2012). It was also found that asexuals were seen in dehumanizing terms by the participants, who labeled them as lacking both “uniquely human” and “human nature” qualities, meaning they were seen as inhuman in both animalistic and machine-like ways (Macinnis & Hodson, 2012). These negative attitudes contribute to interpersonal stigma, a minority stressor."
Passing When Asexual: Methods for Appearing Straight (McKendree University)
“ The research indicated that coming out occurs in liberal spaces and passing occurs in conservative spaces. The findings showed that all but one participant both passed and are out to some extent. The great majority of the participants were out to friends at college, a typically liberal space. This is revealed by the fact that Karen reported that she came out to her college friends because she knew that they would accept her. Emily and Elayne reported similar experiences and reasons for coming out. Conversely, participants showed tendencies to pass at home and in church, both traditionally conservative areas. Families were reported as being less understanding, or at least less knowledgeable, than the environment at school (Emily, Toni, Karen, Sam Interviews). The final analysis of the research indicates a strong sentiment that the information that is available for people new to the asexual community is largely inadequate and difficult to find. This reveals that there is a legitimate need for more widely available information about asexuality, not only for those who are beginning to identify but also for those who do identify as well as families that need to understand. Passing is a perceived necessity that has long been associated with sexual deviance, and minority status (Wallqvist and Lindblom 2015). Understanding how and why asexual people pass is a crucial facet of understanding asexuality as a whole.”
Stories About Asexuality: A Qualitative Study on Asexual Women (Journal of Sex & Maritial Therapy)
"Given that they did not have a name or label to describe how they felt, 4 women thought there must be something wrong with them.With the exception of 2 women, all participants have come out to others, at least partially: they have told other people that they are asexual. Jessica, 30 years old and single, described how she felt forced to come out so she could have a normal relationship with her mother.
Ihadtocomeout,becausenowuhm... nowIcanhaveanormalconversationwithmymother,until that time our conversation only regarded relationships, and then I got angry, and then she got angry and we were both angry. Eventually, all we did was fighting, and that’s why I have decided to come out.
(Jessica, 30 years old, single)
Other women did not feel this pressure but decided to tell people about their asexuality because they had accepted their own identity and wanted to share that with others, given that it is a part of who they are.
It was nice to talk to people about it and to hear: maybe that’s just how it is. Yeah, someone agreeing with me on that, that was really nice.
(Mia, 31 years old, single)
When telling people about their asexuality, the participants in our study received mixed reactions. Five women received negative reactions ranging from not understanding, not believing in the existence of asexuality, to unwanted advice about the necessity to change their asexuality. Emily illustrated these negative reactions prototypically:
Disbelief, like: it’s just a phase, it will change one day, you just haven’t met the right person yet, you just haven’t been truly in love yet. Things like that.
(Emily, 20 years old, in a relationship)While 5 women stated that being asexual did not have a major effect on their currently daily life, 4 participants nevertheless indicated changes since they realized they are asexual. For example, 26-year-old and single Chloe described how it has changed her social life:
I’ve noticed that I less often feel like going out with friends, for instance because then you’re in that situation again and I don’t want that. [ . . . ] While before, I used to love it, going out dancing, but then it didn’ t have that connotation yet. [... ] Now, when I go out and I meet men, I try to stay as neutral as possible.
(Chloe, 26 years old, single)The support of an online community might especially be important given that recent evidence showed that asexual individuals may be viewed more negatively than other sexual minorities (MacInnis & Hodson, 2012). This was also somewhat reflected in the negative and dismissive reactions some of our participants experienced when they came out. Scherrer (2008) and Bogaert (2012) noted that the process of identity development in asexual persons shows similarities with the processes of developing a lesbian, gay, or bisexual identity. The possible parallels in sexual identity development between lesbian, gay, and bisexual individuals and asexual individuals could be informative for clinicians when asexual individuals would consult them. After all, this would imply that asexual persons experience struggles and (minority) stress similar to those of lesbian, gay, and bisexual individuals and that when asexual persons would seek clinical counseling, attention should also be paid to these topics, apart from working toward acceptance of the asexual identity."
“I have a lot of feelings, just none in the genitalia region”: A grounded theory of asexual college students’ identity journeys (Journal of College Student Development)
“This research also brings awareness to pervasive allonormativity and the negative influences asexual invisibility, invalidation, and erasure have in the lives of asexual students. Max provided an important summative comment, “Being invisible isn’t a privilege, and it’s not [pause] I don’t know how to describe it because I feel like it’s too obvious for words in a lot of ways.” Max’s words underscore the narratives of participants who collectively felt they were broken, obstacles to their development, and experiences of oppression fueled by the invisibility of asexuality. These findings align with Robbins et al., (2016) perceptions about invisibility including the unique role of the internet in discovering asexuality and students’ likelihood to pathologize their lack of attraction before gaining awareness of asexuality.
In a 2015 online survey of asexual college students, 70% of participants identified increased awareness of asexuality as a top priority for improving higher education for asexual students (Author, 2015). The findings from this study further illuminate the imperative of asexual visibility. Increased visibility represents a pivotal tool for supporting asexual students in finding and understanding their identities. If students knew asexuality existed, perhaps their journeys gaining awareness of asexuality, could include more personal authority and less feelings of uncertainty and inadequacy. This is not to suggest that visibility is all that institutions should do to support asexual students; rather, acknowledging that asexual students exist and creating awareness represents a necessary foundation to begin deconstructing allonormativity and supporting identity development of asexual students.
In students’ expatiation, the salience of their asexual identities as well as their other identities also influenced their processes and experiences of asexual identity development. The study findings clearly indicate the inextricable connection between asexuality, students’ multiple identities, and the multiple oppressive societal influences. Across the entire ASE model, students’ multiple minoritized identities influenced their identity journey from how they found asexuality, the salience of their asexuality, and how they integrated asexuality within their lives. Students with multiple minoritized identities often engaged in more expansive identity exploration as they tried to put the pieces together inclusive of all of their identities.
Students with multiple minoritized identities discussed ways oppression of their multiple identities, in conjunction with their asexuality, created cumulative marginalization. Of particular note, the experiences of intersectional invisibility described by the Students of Color emphasize lasting effects of whiteness associated with asexuality. The participants in this study did not specifically mention the overt omission of race from AVEN or the historic foundations of asexual as a racialized term; rather, they acknowledged the broad invisibility of asexual People of Color in any contexts they had discovered. Gender and ability stereotypes influenced students’ though the entire model. The experiences of asexual students with multiple minoritized identities underscores the continued importance of not examining students’ identity development in fragmented or isolated ways.
The findings integrating students’ multiple identities align with the findings from Foster et al. (2019) study of asexual WOC. They similarly identified participants’ feelings of isolation, particularly in struggling to find asexual Communities of Color. Within the domain of identity development processes, the ASE model supports several of their findings including experiences of making sense of differences, negotiating personal definitions of asexuality, and acceptance of asexual identity. These similarities highlight areas for continued research centering asexual college Students of Color.”
“Maybe all these random experiences form a cohesive picture”: towards a grounded theory of asexual college students’ identity development (a book-length exploration into the effects of asexuality on twelve college students from The University of Iowa)
“This study explored the experiences of 12 college students as they reflected on their journeys to understand their sexual identities. Each of the students identifies as asexual. In other words, they have little to no sexual attraction to people of any gender. Distinct from celibacy (which is a choice to refrain from sexual behavior), the students described feeling a sense of difference from peers and family during their adolescence. Using an interview-based method, students shared about memorable experiences related to their asexual identity.
From the participants’ experiences, a theory emerged as a potential representation of asexual college student identity development, the Asexual Student Expatiation Model (ASE). The ASE model demonstrates the complexity and non-linearity of the students’ experiences within societal structures that invalidate asexuality. Within the model, students engaged in processes of assimilating, searching for meaning, seeing themselves as asexual, situating in society, internalizing negativity, and experiencing wholeness. The students’ stories detail their unique and individual experiences and paths navigating gaining awareness, identifying, and reconciling asexuality in their lives with their other identities.
The study informs future research, theory, and college student affairs professionals. Recent estimates suggest that more than five percent of college students may identify as asexual. Despite the suggested prevalence, this is the first study of asexual college students that uses their narratives as the foundation for exploration.“
Coming To An Asexual Identity: Negotiating Identity, Negotiating Desire (from Sexualities: Sage Journals)
"As suggested throughout, there are myriad connections between asexuality and other sexual minorities. First, asexuality shares an association both historically and presently to medical institutions with other margin- alized sexual desires and behaviors. Yet, while activists and scholars have challenged the connections between medical discourses and same-sex desire (Conrad and Schneider, 1994; Kraft-Ebbing, 1886 [1959]; Rubin, 1984), diagnoses associated with asexuality (such as Sexual Aversion Disorder and Hyposexual Desire Disorder) are relatively unexplored. These similarities motivate collaboration in political strategy, as both asexual people and other sexual minorities who are in conversation with medical discourses might collaborate for a more complete transformation of these discourses. The lack of visibility and awareness of asexuality is a barrier to its inclusion in other sexuality-based political action groups.While a historical and contemporary relationship with discourses of medicine are shared, LGBTQ identities also have a historical relationship with legal institutions as gender presentation and same-sex behaviors have been prosecuted by legal institutions (D’Emilio, 1983; Rubin, 1984). Asexuality, on the other hand, has been largely unnoticed by legal insti- tutions, perhaps in part because of its lack of behavior and desire. In some ways, because asexuality is defined as a lack of behavior or desire, it has escaped attention, which is a clear departure from the experiences of other marginalized sexualities.
Asexual and LGBTQ groups also share similarities as both have created identity-based communities. As research documents, gay, lesbian, trans- gender and BDSM individuals use sexual identity communities to find support, relationships and to engage politically (D’Emilio, 1998; Rust, 1992). This is similar to how asexual individuals describe the functions of asexual communities. These communities not only serve similar functions, but both asexual and LGBTQ people are using internet technologies to form community (Jay, 2003; McKenna and Bargh, 1998; Turkle, 1995). While both utilize the networking possibilities of the internet, queer communities have additional visibility in physical spaces such as bars, bookstores and social service organizations that cater to LGBTQ ident- ities. Furthermore, there are cultural symbols that represent the desires, identities and behaviors of LGBTQ identities and subcultures (such as rainbows or pink triangles), whereas symbols of asexual identities and and subcultures are not yet generally recognizable. Thus, while both asexual and LGBTQ identities have identity-based communities, the forms and functions of these communities are distinct.
While the aforementioned aspects are more social-structural, asexuality shares a similar social-psychological process of coming to an identity as other marginalized sexual identities. As Paula Rust says, sexual identity is ‘a description of the location of the self in relation to other individuals, groups and institutions’ (Rust, 1996: 78). Given this understanding of sexual identity, bisexual, asexual, gay and pan-sexual individuals all draw on existing language, their current social situation and the social and cultural meanings associated with these identities to place themselves in relation to other individuals and institutions and to accurately describe their internal sense of self. Additionally, asexual individuals, as well as gay, bisexual or queer individuals, often share a sense of their sexuality as biological and innate, despite descriptions of coming to these identities that reveal profoundly social experiences.
In this article, I have described a few of the intersections between asexuality and other marginalized sexualities. This analysis is far from exhaustive, but it highlights the similarities between these sexualities and creates a need for further exploration of the overlapping social and political agendas of these marginalized sexualities. Not only are asexual identities interesting in their own right, but they contribute to a broader understanding of the construction of sexualities."